
Getting to Know the Patient

The case described above in Getting to Know the Patient was unusual because it involved talking a cataract patient out of selecting a premium IOL, rather than into one. First, a little background on my regional situation is in order.
A STATE OF CHANGE
The Swedish public health care system is currently in a state of change regarding access to premium IOLs. Previously, only monofocal aspheric and spherical IOLs were available to cataract patients, who paid the regular fee for a doctor visit of around €30 when they had their cataract surgery (and no extra fee if both eyes were operated on the same day). In recent years, patients in some counties of Sweden, after decisions in their local parliaments, can pay extra to have a toric or multifocal IOL implanted at their cataract operation. (See my previous article, “Copayments Don’t Really Matter in Public Health Care,” on page 50 of the September 2015 issue of CRST Europe.)
In my county (Östergötland), this policy has not yet been implemented. Swedish law allows citizens to seek health care wherever they wish in Sweden, so they may choose to travel to a county with more access to premium IOLs. Only a fraction of 1% of patients makes that choice. Another group of patients may choose to have their surgery at a private clinic and pay the whole cost out of pocket, in which case they have access to any premium solution that fits their situation and meets their expectations.
In 2014, after a public bidding process in my county, two one-piece IOLs for in-the-bag implantation were made available for routine use in our clinic; one is an aspheric, aberration-neutral hydrophilic acrylic IOL with a modified surface to prevent development of posterior capsular opacification, and the other is an aspheric aberration-correcting hydrophobic acrylic IOL in a preloaded system.
IOL choice is made by each surgeon, based on which IOL he or she feels more comfortable implanting. In cases in which a patient has been previously operated in the other eye, an IOL of similar optical design may be chosen to match the one already implanted.
CHOOSING TO STAY LOCAL
After discussing the alternatives—operation elsewhere with a toric IOL, or operation in the home county clinic with implantation of an aspheric monofocal IOL—the patient decided to accept the latter.
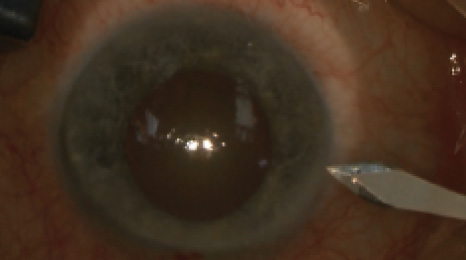
Figure 1. A 1.8-mm incision is created at the steep meridian.
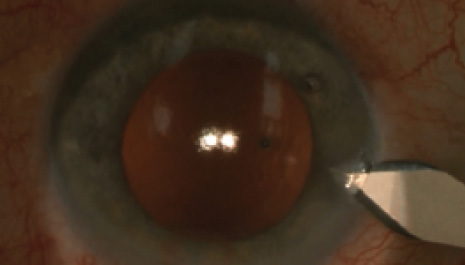
Figure 2. With OVD expanding the anterior chamber and capsular bag, the phaco incision is widened to 2.75 mm.
Surgery was planned and performed with the phaco tunnel placed in the steep meridian, at 170°. Before placing the IOL, the 1.8-mm phaco tunnel (Figure 1) was widened with a 2.75-mm steel slit-knife (Figure 2), which was also used to create an opposite limbal incision at 350° with the same construction as the phaco tunnel (Figure 3). A monofocal, nontoric, aspheric, aberration-correcting, one-piece, hydrophobic acrylic IOL was comfortably implanted through the widened tunnel into the capsular bag. The phaco tunnel was hydrated to ensure a tight wound at the end of surgery. No hydration was necessary in the opposite limbal incision (Figure 4).
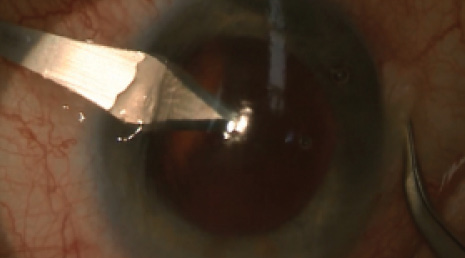
Figure 3. A clear corneal incision of 2.75 mm is made opposite the phaco incision.
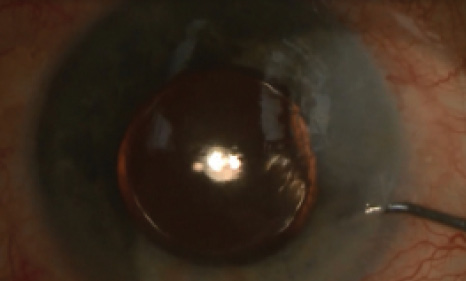
Figure 4. At the end of surgery, only the phaco incision needs hydrating to ensure watertightness.
Six weeks after the operation, at the patient’s scheduled follow-up, his UCVA was 0.7 OS, and BCVA with refraction of plano -0.75 X 55° was 0.8. Ten weeks later, both his visual acuities and refraction remained the same. The patient was happy and enjoyed the improved vision, especially at the golf course.
A GOOD REMINDER
Case Recap
Who
69-year-old man with cataract and possible meridional amblyopia in his left eye, requesting referral to another county to receive a toric IOL (unavailable in his home county)
What
Deciding between undergoing cataract surgery elsewhere with a toric IOL or in the home county clinic with implantation of an aspheric monofocal IOL, which had potential to provide a significant decrease in the patient’s refractive cylinder
How
Despite not receiving the IOL he had hoped for, the patient was satisfied with his results after implantation of the aspheric monofocal IOL in his home clinic (UCVA, 0.7; BCVA, 0.8, with a significant reduction of preoperative astigmatism)
I chose to report on this case as a reminder that, even considering the continual advances in IOL optical design and the ever-expanding possibilities to offer patients a variety of solutions for their individual refractive situations, we still can provide patients with a satisfactory outcome when the selection of IOLs available in a country, region, or county is limited.
Although I do believe that toric IOLs, the latest technologies, and the time required to optimally use them are important investments to improve the quality of life of our patients, surgeons should always aim to work with whatever tools are available to them to find the best solution for their patients. n
Björn Johansson, MD, PhD, FEBO
• Associate Professor, Department of Ophthalmology, Linköping University, Sweden
• Member, CRST Europe Editorial Board
• bjorn.johansson@regionostergotland.se
• Financial interest: None acknowledged