
SMILE is on the Spot
Goodbye excimer laser, hello femtosecond laser.
By Bertram Meyer, MD
Since 2011, our clinic has performed more than 1,800 ReLEx small incision lenticule extraction (SMILE) procedures using the VisuMax femtosecond laser (Carl Zeiss Meditec) in myopic and myopic-astigmatic eyes with spherical equivalents between -0.75 and -10.00 D. The clinical outcomes have been outstanding and even slightly better that those we have achieved with femtosecond LASIK (femto-LASIK): At 3 months, more than 92% of eyes are within ±0.50 D of target (Figure 1).
In fact, we have now moved to offering SMILE in preference to LASIK. We performed a retrospective analysis of all our refractive laser patients in 2014 and found that 82.2% of these patients were suitable candidates for SMILE. And, of these patients, 98.4% elected to undergo that procedure. Why is that? Patients appreciate that the SMILE procedure is painless, bladeless, and flapless. The key reason for their choice of SMILE over LASIK is the fear of flap creation and healing with LASIK. Moreover, patients appreciate that SMILE is a fast procedure independent of the amount of refractive error corrected, and that it is completed in a single step, without a shift from one laser to another. The complete surgery, including manipulation of the lenticules, is done with the VisuMax femtosecond laser (Carl Zeiss Meditec) in less than 10 minutes for both eyes. There has been no reported risk of haze or diffuse lamellar keratitis.
Since we have begun performing SMILE, our rate of refractive laser procedures has increased more than 40%, despite the fact that we charge a significantly higher price for SMILE than for traditional femto-LASIK. We believe that, with SMILE, we are offering an extraordinary refractive procedure that distinguishes our clinic from others.
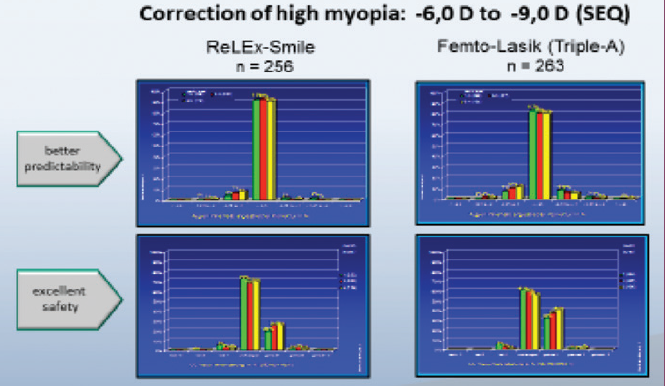
Figure 1. SMILE versus femto-LASIK in high myopia. Courtesy of Bertram Meyer, MD
HIGH PRECISION
The high-precision optics and curved contact glass of the VisuMax laser enable extremely precise 3-D cuts and the preparation of wavefront-optimized lenticules within a closed system. This makes the procedure independent of external influences such as temperature, humidity, airflow, and debris absorption, and also independent of hydration of tissue and the corneal bed. Due to the accuracy of the femtosecond laser, the predictability of refractive outcomes is excellent, especially in higher ranges of correction. There is no waste of tissue, as there is no need for transition zones. Moreover, SMILE has the advantage that we are cutting not a flap but a cap. Consequently, the integrity and mechanical stability of the anterior cornea and the corneal surface tension are well preserved. Without a flap, related complications such as striae, dislocation, and epithelial ingrowth cannot occur. Furthermore, dry eye syndrome is less frequent postoperatively because fewer corneal nerves are damaged during SMILE.1,2
There is excellent stability of results over time and safety regarding BCVA. Admittedly, however, recovery of postoperative visual acuity takes slightly longer after SMILE than conventional femto-LASIK.
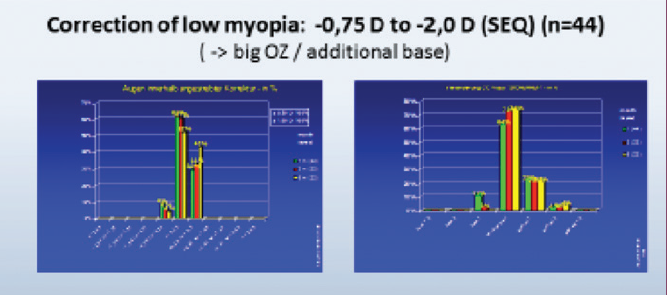
Figure 2. SMILE in low myopia.
.
Postoperative corneal topography shows a large and homogeneous optical zone with a slightly prolate corneal shape. The achieved effective optical zone is identical to the laser setting, independent of the degree of refractive correction. Wavefront measurements have confirmed that there is no significant change in aberrations from before to after surgery, and, specifically, no spherical aberration is induced by lenticule creation and extraction.
SMILE has also become an excellent option for treatment of low myopia. We have performed SMILE on eyes with myopia as low as -0.75 to -2.00 D. To simplify the management of the thin lenticule in these eyes we have used a larger optical zone (7 mm) and added an additional refraction-neutral corneal tissue base. Safety and refractive outcomes are excellent (Figure 2).
WHY DO PATIENTS PREFER SMILE?
As noted above, a large percentage of our refractive surgery patients have opted for SMILE since we began offering it. With information obtained on the Internet and through social media, more patients are aware that the LASIK flap never completely heals and that nowadays almost all LASIK complications and problems are flap-related.
Consequently, no flap means maximum safety. Patients can go back to normal life on the next postoperative day, and all sorts of sporting activities—even including physical contact—are allowed. Due to the large optical zones and less induced spherical aberration, patients complain less about problems driving at night.
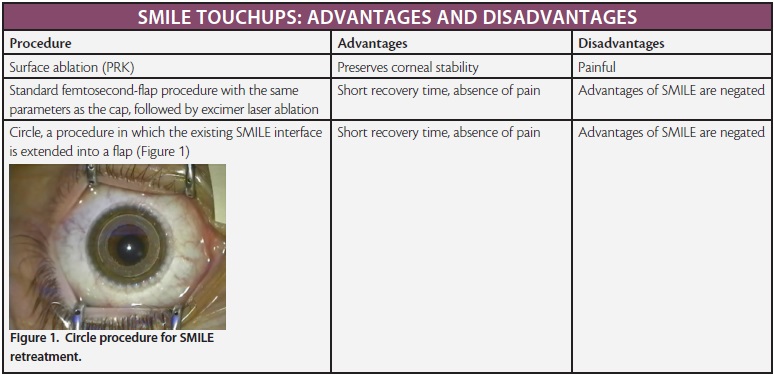
Retreatments after SMILE are rare, with a rate of about 2% in our practice. The reason is the stability of refractive outcomes and high tolerance among patients for small refractive errors postoperatively. If a touchup is required, we have several options to choose from (see SMILE Touchups: Advantages and Disadvantages).
SUMMARY
SMILE is a minimally invasive keyhole procedure that combines excellent refractive and visual outcomes with maximum safety. To round out its range of correction, treatment of myopia of greater than -10.00 D and of hyperopia are currently being investigated.
1. Li M, Zhao J, Shen Y, et al. Comparison of dry eye and corneal sensitivity between small incision lenticule extraction and femtosecond LASIK for myopia. PLoS One. 2013;8(10):e77797.
2. Xu Y, Yang Y. Dry eye after small incision lenticule extraction and LASIK for myopia. J Refract Surg. 2013;30(3):186-190.
Why I Offer SMILE and LASIK
The all-femtosecond procedure is the preferred option, but excimer-based surgery is still useful in eyes with low hyperopia or mixed astigmatism and older patients with presbyopia.
By Sri Ganesh, MBBS, MS, DNB
About 3 years ago, I had a cluster of patients who experienced post-LASIK ectasia. On reviewing their preoperative data and topographies, they all seemed to be ideal candidates with a low risk of ectasia. I have been performing LASIK for the past 18 years and femto-LASIK for the past 6, with a total of more than 40,000 procedures completed to date. The realization that ectasia can occur in a small percentage of patients, even with thorough preoperative screening and patient selection, made me rethink the safety that LASIK offers.
Many of my colleagues around the world have shifted away from LASIK to predominantly performing surface ablation procedures in low myopia and in younger patients. However, the discomfort, delayed healing time, and prolonged medication regimen associated with surface ablation did not make this a more appealing alternative to me.
It was at this time that I started reviewing the technology and results of the SMILE procedure, and I decided to adopt this technology into my practice. For the past 2.5 years, I have mainly been performing SMILE and have refined my technique and results. I have found numerous advantages of this technique in terms of safety, results, and patient satisfaction.1 There are also advantages to the surgeon and the surgery center in terms of higher revenue per procedure; better marketability of this bladeless, flapless procedure; and increase in patient inflow.
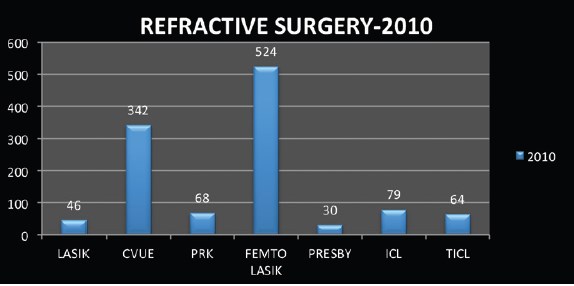
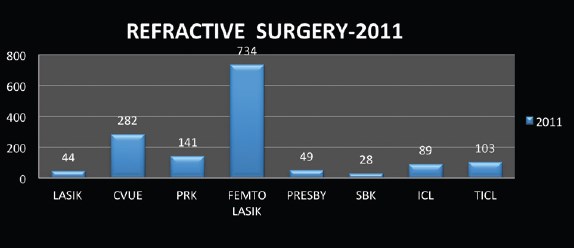
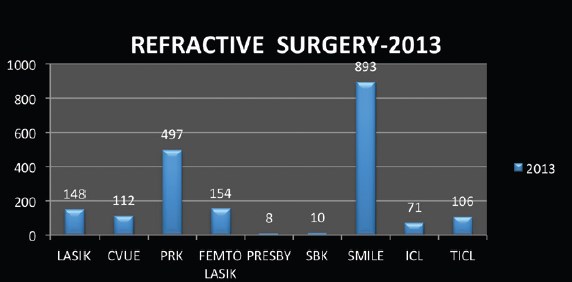
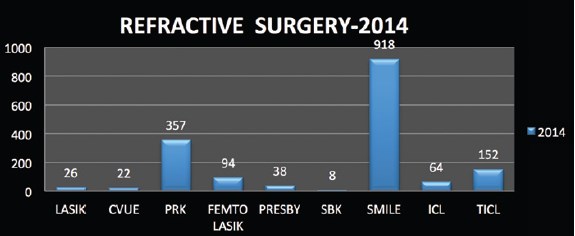
Figure 3. Numbers of refractive procedures performed in the past 5 years. CVUE = CustomVue; SBK = sub-Bowman keratomileusis; TICL = toric ICL. Courtesy of Sri Ganesh, MBBS, MS, DNB
At a Glance
- Patients appreciate that the SMILE procedure is painless, bladeless, and flapless.
- SMILE has the advantage over LASIK that there is a cap and that the integrity and mechanical stability of the anterior cornea and the corneal surface tension are preserved.
- Excimer laser procedures are helpful to treat eyes with low hyperopia or mixed astigmatism, for enhancement in eyes that have residual refractive errors after SMILE, in patients who require customized ablation or hyperopic or presbyopic correction, and in therapeutic indications for PTK.
- Offering multiple laser vision correction platforms increases the range of patients one can treat and for whom one can provide spectacle-free vision.
EXCIMER STILL USEFUL
I still need the excimer laser, however, to treat eyes with low hyperopia or mixed astigmatism and for enhancement in eyes that have residual refractive error after SMILE. The excimer laser is also useful in treating older patients with presbyopia. We use the MEL90 excimer laser (Carl Zeiss Meditec) with Presbyond software coupled with the VisuMax for flap creation in such cases. The MEL90 also has facility to perform topography-linked customized ablations, which is useful for treating irregular corneas.
Most patients undergoing femto-LASIK are presbyopic, and for them I offer laser blended vision correction. This increases the range of patients I can treat and for whom I can provide spectacle-free vision. My results with Presbyond over the past year have been gratifying, with good patient satisfaction and binocular functional vision for distance, intermediate, and near. I also offer excimer laser surface ablation for patients with low myopia who cannot afford the higher-priced SMILE procedure.
PROCEDURE OF CHOICE
On reviewing my data on refractive surgeries performed in the past 5 years (Figure 3), SMILE is now the most often performed procedure, and the number of SMILE procedures has increased yearly since we began offering it in 2012. I also find that, although the patient’s cost for the procedure is considerably higher than that for LASIK, the total volume of refractive procedures has also increased in the past 3 years. This translates directly into increased revenue for the practice and reflects our patients’ confidence in undergoing refractive procedures at our center.
SMILE is my procedure of choice to treat myopia and myopic astigmatism of up to -10.00 D, and I strongly believe that this technique is the future of refractive surgery. With that said, I still find that the excimer laser is helpful to treat patients who require customized ablation or hyperopic or presbyopic correction, and also in therapeutic indications for PTK. In the end, I foresee the use of the excimer laser for refractive surgery declining in the years to come, and I believe it will largely be replaced by femtosecond technology and lenticule extraction approaches. n
1. Ganesh S, Gupta R. Comparison of visual and refractive outcomes following femtosecond laser- assisted lasik with smile in patients with myopia or myopic astigmatism. J Refract Surg. 2014;30(9):590-596.
Bertram Meyer, MD
- Eye Center Cologne, Cologne, Germany
- meyer@augencentrumkoeln.de
- Financial disclosure: Consultant (Carl Zeiss Meditec)
Sri Ganesh, MBBS, MS, DNB
- Chairman and Managing Director, Nethradhama Super Specialty Eye Hospital, Karnataka, India
- chairman@nethradhama.org
- Financial disclosure: None