
The introduction of the femtosecond laser has yielded increased safety and accuracy in the field of refractive surgery.1,2 However, one specific complication, the opaque bubble layer (OBL), has arisen with its use. This phenomenon can occur during either femtosecond LASIK (femto-LASIK) or ReLEx small incision lenticule extraction (SMILE).3 Studies have reported that an OBL tends to develop in thicker corneas during femto-LASIK.4,5 At the same time, central corneal thickness is positively correlated with corneal biomechanics.6 Studies concerning the OBL during SMILE surgery, however, are rare.
This article, which presents several cases in which an OBL developed during SMILE, is intended to explore the influence of corneal biomechanics on the incidence of this complication.
CASE PRESENTATIONS
All patients described in this article underwent preoperative examinations including UCVA, BCVA, manifest and cycloplegic refraction, noncontact IOP measurement, anterior segment slit-lamp microscopy, corneal topography with a Scheimpflug tomography system (Pentacam; Oculus Optikgeräte), and preoperative measurement of corneal biomechanics including corneal resistance factor (CRF) and cornea hysteresis (CH) using the Ocular Response Analyzer (ORA; Reichert Technologies). For the ORA examination, three to four records with a signal score greater than 3.5 were obtained for each eye, and the average values of CRF and CH were calculated.
All SMILE procedures were performed on the same day with the same treatment protocol. The femtosecond laser used for the procedure (VisuMax; Carl Zeiss Meditec) has a 500-kHz repetition rate with 150-nJ energy delivered per pulse. The thickness of the corneal cap was uniformly 120 µm, the diameter of the corneal cap was 7.5 mm, the diameter of the lenticule was 6.5 mm, and all sidecut angles were 90°.
The femtosecond laser scanned to create the lenticule in proper sequence: (1) the posterior surface, (2) the edges, (3) the anterior surface, and (4) the sidecut incision. A 3-mm incision was created at the 12-o'clock position at the edge of the corneal cap, and a basement of 10 μm for the lenticule was set in order to successfully remove the lenticule. After surgery, patients applied 0.3% topical ofloxacin (Tarivid; Santen) four times daily for 2 days and 0.1% fluorometholone (Flumetholon; Santen) four times daily for 2 weeks, then decreased one time every 2 weeks and discontinued over
2 months postoperatively.
Case No. 1. A 24-year-old patient presented with a refraction of -3.75 -1.00 X 175º OD and -3.25 -1.00 X 175º OS. Preoperative central corneal thickness was 526 μm OD and 522 μm OS. The preoperative averaged CRF and CH were 8.53 and 8.77 mm Hg OD and 8.35 and 9.7 mm Hg OS, respectively. Almost no OBL occurred during the creation of the posterior surface of the lenticule in both eyes. During the scanning of the anterior surface, however, slight OBL occurred in the middle of the lenticule (see Case No. 1).
AT A GLANCE
- The complication of OBL has arisen with the use of the femtosecond laser during both femto-LASIK and ReLEx SMILE.
- Considering the mechanism of OBL, the authors hypothesize that thicker corneas with better corneal biomechanics are more likely to develop OBL during SMILE.
- Further clinical study with larger numbers of eyes is needed to determine the effect of corneal biomechanics on the OBL during SMILE.
Case No. 2. A 22-year-old patient presented with a refraction of -4.25 D in both eyes. Preoperative central corneal thickness was 561 μm OD and 565 μm OS. The preoperative averaged CRF and CH were 9.33 and 10 mm Hg OD and 9.87 and 10.53 mm Hg OS, respectively. Slight OBL at the periphery of the posterior of the lenticule and moderate OBL at the center of the posterior surface of the lenticule were observed (see Case No. 2).
Case No. 3. A 22-year-old patient presented with a refraction of -3.25 -0.25 X 180º OD and -2.75 -0.75 X 175º OS. Preoperative central corneal thickness was 575 μm OD and 581 μm OS. The preoperative averaged CRF and CH were 11.67 and 10.80 mm Hg OD and 11.03 and 10.97 mm Hg OS, respectively. Moderate OBL occurred at the periphery of the posterior of the lenticule, and severe OBL developed in the center of the posterior surface of the lenticule (see Case No. 3).
CASE NO. 1
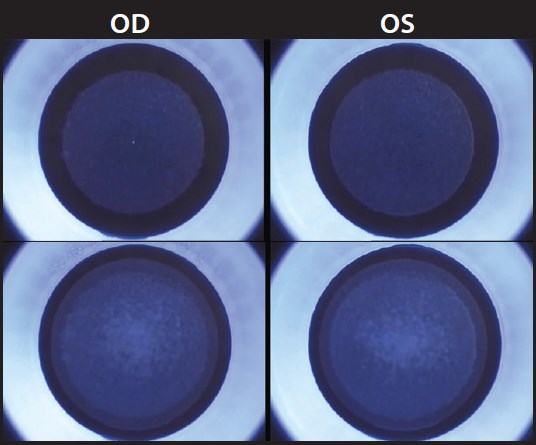
No OBL at the posterior surface and slight OBL at the anterior surface of the lenticule (OD and OS).
CASE NO. 2
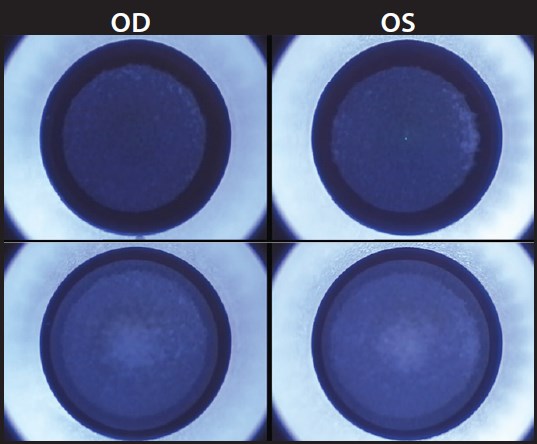
Slight and moderate OBL at the posterior and anterior surfaces of the lenticule, respectively (OD and OS).
CASE NO. 3
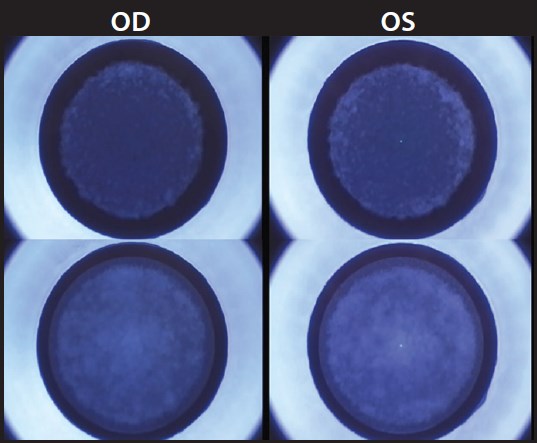
Moderate and severe OBL at the posterior and anterior surfaces of the lenticule, respectively (OD and OS).
DISCUSSION
The effect of the OBL on visual outcomes is controversial. Clinical experience has shown that excessive OBL may interfere with the penetration of femtosecond laser pulses and may gather at the edge of the lenticule, resulting in difficult tissue separation and residual marginal lenticule.7 Studies have reported that thicker corneas tend to develop an OBL during femto-LASIK.4,5
Considering the mechanism of OBL, it is hypothesized that thicker corneas might also tend to develop an OBL during SMILE. Similarly, central corneal thickness may be positively correlated with corneal biomechanics in SMILE, as it is in LASIK.6
The femtosecond laser creates corneal resection by delivering laser pulses to induce a plasma of approximately 1 to 5 mm diameter at a predetermined corneal depth. The expanding of the plasma is accompanied by the generation of an impulse wave and creation of a gas bubble (carbon dioxide) and water, which, in turn, cleaves the tissue and creates a plane of separation.5 Then the carbon dioxide and water are absorbed by the surrounding tissue and the pump function of the endothelial cells. The OBL is a collection of gas bubbles in the intralamellar spaces of the cornea. It is generated by the diffusion of the bubble of carbon dioxide and water to the anterior or the posterior surface of scanned tissue through the gaps created between collagen fibers.
Theoretically speaking, the gas bubbles produced by the femtosecond laser travel the pathway of least resistance.8 Because the posterior cornea has less interweaving of lamellae than the anterior cornea, the posterior cornea is weaker, and it is easier for the posterior tissue to be cleaved and for the gas bubble to be absorbed; in stronger tissue, the gas bubbles are under higher pressure due to corneal compression and high vacuum, and it is easier for the bubbles to diffuse to the anterior or the posterior surface of the scanned tissue to generate an OBL. From this point of view, weaker corneal biomechanics may be beneficial for the prevention of OBL. We theorize that this is why an OBL did not occur at the posterior surface but did occur at the anterior surface of the lenticules in case No. 1.1
Regarding corneal biomechanics, the posterior two-thirds of the stroma in the periphery of the cornea is stronger than the posterior two-thirds stroma in the central cornea,7 and this is consistent with the fact that OBL occurred only at the edge of the posterior surface of the lenticule in cases Nos. 2 and 3.
Comparing the three cases presented here, the thicker the central cornea and the higher the CRF and CH values, the more severe the OBL observed at both the posterior and anterior lenticule surfaces. This phenomenon also suggests that corneas with greater rigidity and more resistance are more likely to restrict the clearance of gas bubbles and increase the occurrence of OBL.4
CONCLUSION
From the analysis of the three cases presented here, it may be hypothesized that, during SMILE, a cornea with stronger biomechanics is more likely to experience OBL. The OBL also tends to occur at the edge of the posterior and anterior surfaces of the lenticule. Further clinical study with larger numbers of eyes is needed to confirm this hypothesis. n
1. Stonecipher K, Iagnacio TS, Stonecipher M. Advances in refractive surgery: microkeratome and femtosecond laser flap creation in relation to safety, predictability, and biomechanical stability. Curr Opin Ophthalmol. 2006;17(4):368-372.
2. Santhiago MR, Kara-Junior N, Waring GO 4th. Microkeratome versus femtosecond flaps: accuracy and complications. Curr Opin Ophthalmol. 2014;25(4):270-274.
3. Wang Y, Wu Z, Tang X, et al. Two millimeter micro incision lenticule extraction surgery with minimal invasion: a preliminary clinical report [article in Chinese]. Zhonghua Yan Ke Za Zhi [Chinese Journal of Ophthalmology]. 2014;50:671-680.
4. Liu CH, Sun CC, Hui-Kang Ma D. Opaque bubble layer: Incidence, risk factors, and clinical relevance. J Cataract Refract Surg. 2014;40(3):435-440.
5. Kaiserman I, Maresky HS, Bahar I, Rootman DS. Incidence, possible risk factors, and potential effects of an opaque bubble layer created by a femtosecond laser. J Cataract Refract Surg. 2008;34:417-423.
6. Roberts CJ. Concepts and misconceptions in corneal biomechanics. J Refract Surg. 2014:40:862-869.
7. Wang Y, Zhao K. Refractive Surgery with Femtosecond Laser. Beijing: People's Medical Publishing House. 2014:116-118.
8. Hurmeric V, Yoo SH, Fishler J, Chang VS, Wang J, Culbertson WW. In vivo structural characteristics of the femtosecond LASIK-induced opaque bubble layers with ultrahigh-resolution SD-OCT. Ophthalmic Surg Lasers Imaging. 2010;41:109-113.
Rui Dou, MD
- Ophthalmologist, Tianjin Eye Hospital & Eye Institute, Tianjin Key Lab of Ophthalmology and Visual Science, Tianjin Medical University, Tianjin, China
- dourui0718@126.com
- Financial disclosure: None
Yan Wang, MD, PhD
- Professor, Tianjin Eye Hospital & Eye Institute, Tianjin Key Lab of Ophthalmology and Visual Science, Tianjin Medical University, Tianjin, China
- wangyan7143@vip.sina.com
- Financial disclosure: None