

Figure 1. In Circle, a lamellar ring is created at the same depth as the existing SMILE incision, allowing the conversion of the SMILE cap into a hinged flap. The flap is then raised, and excimer laser ablation is performed.
MANAGING COMPLICATIONS
The Three Phases of SMILE
Phase 1: Initial docking with precise centration. During this phase, proper head position is achieved by tilting the patient's head medially to avoid nasal contact with the cone of the contact glass interface. Precise centration should be verified before the initiation of suction.
Phase 2: Femtosecond laser delivery. Femtosecond laser pulses are fired in a spiral pattern with a pulse energy of 120 to 170 nJ and a repetition rate of 500 kHz.
Phase 3: Tissue dissection and lenticule removal. The tissue disruption planes created by the laser include the posterior lenticule surface, vertical edge cut, anterior lenticule surface, and corneal sidecut (Figures 1 and 2).

Figure 1. Cross-section of the cleavage planes created during SMILE: (1) posterior lenticule surface, (2) vertical edge cut, (3) anterior lenticule surface, and (4) corneal sidecut.

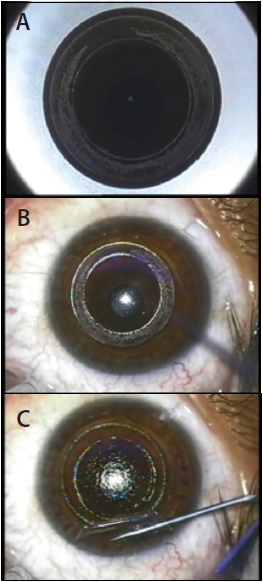
Figure 2. Surgical steps of the SMILE procedure, including laser-assisted and manual steps. Laser-assisted: posterior tissue disruption plane, or lenticule cut (A); anterior tissue disruption plane, or flap cut (B); superior flap and sidecut incision (C). Manual steps: delineation of planes (D), dissection of planes (E), and lenticule removal (F).
SMILE OVER LASIK
enhancement technique
1. Sekundo W, Kunert K, Russmann C, et al. First efficacy and safety study of femtosecond lenticule extraction for the correction of myopia: 6 month results. J Cataract Refract Surg. 2008;34:1513-1520.
2. Sekundo W, Kunert K, Blum M. Small incision corneal refractive surgery using the small incision lenticule extraction (SMILE) procedure for the correction of myopia and myopic astigmatism: results of a 6 month prospective study. Br J Ophthalmol. 2011;95:335-339.
3. Shah R, Shah S, Sengupta S. Results of small incision lenticule extraction: all-in-one femtosecond laser refractive surgery. J Cataract Refract Surg. 2011;37:127-137.
4. Wong CW, Chan C, Tan D, et al. Incidence and management of suction loss in refractive lenticule extraction. J Cataract Refract Surg. 2014;40:2002-2010.
5. Li X, Wang Y, Duo RV. Aberration compensation between anterior and posterior corneal surfaces after small incision lenticule extraction and femtosecond laser-assisted laser in-situ keratomileusis. Ophthalmic Physiol Opt. 2015;35(5):540-541.
6. Gyldenkerne A, Ivarsen A, Hjortdal JØ. Comparison of corneal shape changes and aberrations induced by FS-LASIK and SMILE for myopia. J Refract Surg. 2015;31(4):223-229.
7. Wu D, Wang Y, Zhang L, Wei S, Tang X. Corneal biomechanical effects: small-incision lenticule extraction versus femtosecond laser–assisted laser in situ keratomileusis. J Cataract Refract Surg. 2014;40:954-962.
8. Sinha Roy A, Dupps WJ Jr, Roberts CJ. Comparison of biomechanical effects of small-incision lenticule extraction and laser in situ keratomileusis: finite-element analysis. J Cataract Refract Surg. 2014;40:971-980.
Mahipal Sachdev, MD
• Chairman, Medical Director, and Senior Consultant
Ophthalmologist, Centre For Sight, New Delhi, India
• drmahipal@gmail.com
• Financial disclosure: Travel grant (Carl Zeiss Meditec)