
Descemet membrane endothelial keratoplasty (DMEK) is the newest and most advanced form of endothelial keratoplasty. It offers unprecedented visual rehabilitation, low rejection rates, and low frequency of postoperative complications.1 Although many cornea specialists consider it to be the new gold standard for treating endothelial diseases, others hesitate to make the transition to DMEK because of the technique’s reputation as being too challenging for the average cornea surgeon.
In response to this sentiment—and to make the operation both easier and less intimidating—we recently standardized the technique and described all steps in detail.2,3 This article focuses on the five keys to no-touch DMEK that cornea specialists starting out with DMEK may especially want to bear in mind.
Fundamental 1. OBTAINING A SOFT EYE
Intraoperative posterior (vitreous) pressure is the main cause of complicated tissue handling during this surgery because, with the anterior chamber compressed or collapsed from below, all of the necessary unrolling and manipulation steps become more challenging.2,3 In order to achieve a soft eye, four actions may be considered: (1) position the surgical bed in an anti-Trendelenburg position; (2) perform manual ocular massage for 2 to 3 minutes; (3) perform oculopressure with a Honan balloon for another 10 to 15 minutes; and (4) during surgery, monitor the tightness of the eyelid speculum and release the speculum tension if the anterior chamber becomes shallow or if any signs of vitreous pressure are observed.
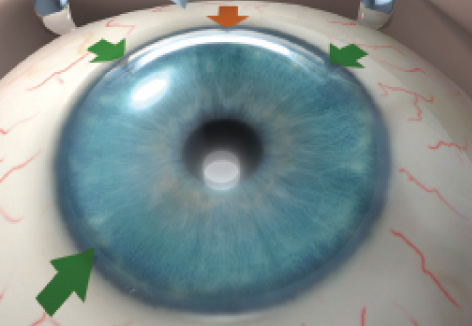
Figure 1. Incisions used in no-touch DMEK: The main incision at the 12-o’clock position (orange arrow) and sideport incisions at the 10:30-, 1:30-, and 7:30-o’clock positions in a right eye or the 4:30-o’clock position in a left eye (green arrows).2
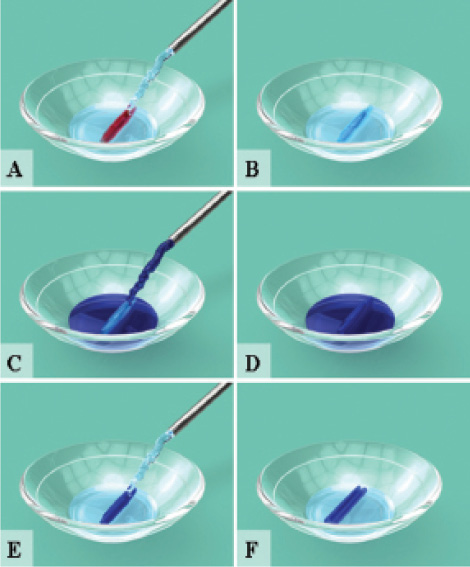
Figure 2. Illustrations show the steps in the final preparation of the DMEK graft in the OR (A-F).2
Fundamental 2. DESCEMETORRHEXIS AND GRAFT PREPARATION
Descemetorrhexis. At the 12-o’clock position, the main limbal incision is marked: that is, dissected to a depth of 50% and a width of 3 mm using a keratome blade. Three sideport incisions are created using a surgical knife: two at the 10:30- and 1:30-o’clock positions and the third at the 7:30-o’clock position in a right eye or at the 4:30-o’clock position in a left eye (Figure 1). With a 30-gauge cannula inserted through a sideport incision, the anterior chamber is completely filled with air. Under air, the recipient Descemet membrane is scored over 360° using a reversed Sinskey hook.2 During descemetorrhexis, the tissue removal may be done under air to avoid leaving any remnant of recipient Descemet membrane that can affect visual outcomes and/or graft adherence.4 After descemetorrhexis, the main incision is completed and the recipient Descemet membrane is removed.
At a Glance
• DMEK, the newest and most advanced form of endothelial keratoplasty, offers unprecedented visual rehabilitation, low rejection rates, and low frequency of postoperative complications.
• No-touch DMEK can be an easy-to-learn and reproducible technique, even for beginning surgeons.
• DMEK may have additional advantages in regions where resource shortages or costs are particular concerns, as the procedure can be performed in virtually any clinical setting without any specialized or expensive equipment.
Preparation of the DMEK graft. The DMEK graft is ideally prepared in an eye bank prior to surgery by stripping the tissue from a donor sclerocorneal rim with a minimum cell count of 2,300 cells/mm2. The tissue is stored for 1 or 2 weeks in a glass vial in organ culture at 31o C.5 At the time of surgery, the content of the glass vial is poured into a glass bowl, and a glass pipette is used to drain the culture medium from the bowl, avoiding any contact with the graft (Figure 2). In the bowl, the DMEK roll is thoroughly rinsed (two to three times) with balanced saline solution (saline) until all visible culture medium residue is removed. The DMEK roll is then stained with trypan blue dye 0.06% for about 30 seconds, rinsed with saline, and again stained with trypan blue dye to obtain an intense blue tissue coloration in order to ensure visibility of the graft in the recipient anterior chamber. The DMEK roll is then rinsed again with saline to remove all excess dye.
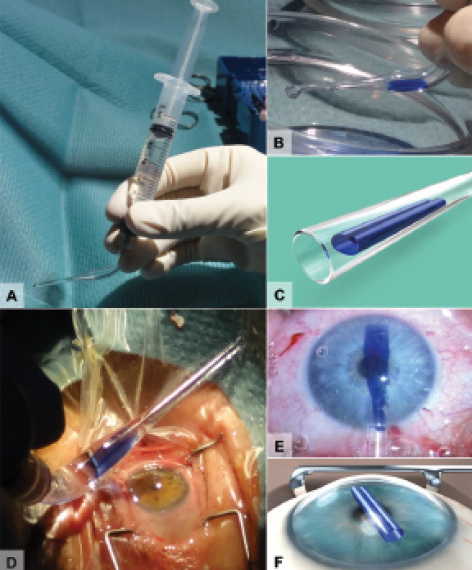
Figure 3. Illustrations and clinical images show steps in the insertion of the DMEK graft (A-F).3
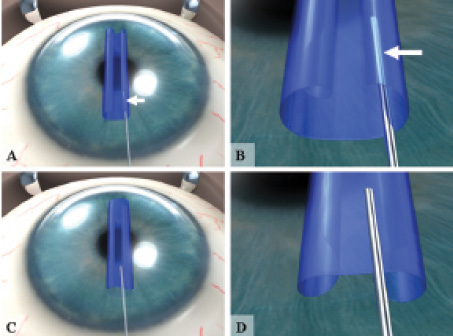
Figure 4. The Moutsouris sign indicates correct graft orientation. If the graft is oriented correctly (A), the tip of the cannula turns blue (B); if not (C), the tip does not turn blue (D).2
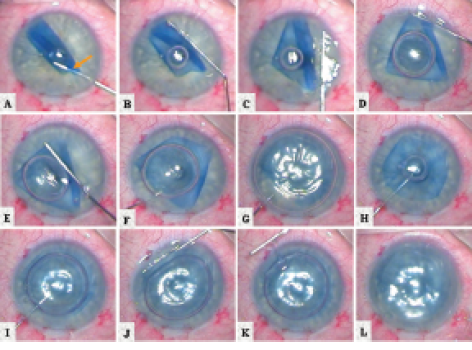
Figure 5. Clinical images show the steps in centration and unfolding of a DMEK graft within the anterior chamber (A-L).2
Freely floating in the glass bowl, the DMEK graft may assume either a single- or double-roll configuration. Because the operation is easier to perform if the tissue is injected into the eye as a double roll, single rolls should be converted into double rolls. This can be done with light irrigation across the tissue surface. By sending a few gentle jets of saline on top and down the length of a single roll, the tissue can usually be encouraged to unscroll and then recurl into a double-roll configuration that is ready for implantation.
Fundamental 3. IMPLANTATION OF THE GRAFT
The stained DMEK roll is sucked into a custom-made glass injector (DORC International). Under the surgical microscope, the orientation of the DMEK graft as a double roll facing upward is verified (Figure 3). In Figure 3, note that the endothelial cells are located on the outer surface of the roll. For this reason, it may be advisable to avoid the use of plastic IOL insertion cartridges and to use to glass injectors instead, as glass surfaces are much smoother. Using the glass injector, the DMEK roll is then inserted into the anterior chamber through the main incision at the 12-o’clock position.2,3
Fundamental 4. ORIENTING AND UNFOLDING THE DMEK GRAFT
The orientation of the graft in the anterior chamber may be checked by positioning the tip of a 30-gauge cannula on top of the membrane and underneath one of the peripheral curls. If the graft is correctly oriented (endothelium facing toward the iris), the tip of the cannula will become slightly blue (Moutsouris sign; Figures 4A and 4B). If the graft is oriented upside-down (endothelium facing the cornea), the tip of the cannula will not turn blue (Figures 4C and 4D), and the graft may be reoriented by gently irrigating it within the anterior chamber.2 Once the graft is turned over, its orientation may be confirmed again using the Moutsouris sign. Obtaining correct orientation is an essential step: If the endothelium is positioned upward (facing the stroma) instead of downward (facing the iris), the DMEK graft will be prone to detachment in the early postoperative phase.
Special care should be taken during manipulation of the DMEK graft using irrigation because the thin graft can easily be flushed out of the eye if the anterior chamber is over-pressurized. For this reason, all manipulation of the graft inside the eye should take placing using one of the sideports, not the main incision.
Once the DMEK graft is correctly oriented, a small air bubble is injected between the double rolls on top of the membrane (Figure 5). The air bubble will be caught between the rolls, and it may be manipulated to further unfold the graft by, in effect, rolling the air bubble on top of the membrane, using a cannula on the outer corneal surface.6 When the graft is further unfolded, the air bubble may be enlarged until the central portion of the DMEK graft is flattened over the iris.
Fundamental 5. POSITIONING AND FIXATING THE DMEK GRAFT
The air is aspirated from the anterior chamber while the tip of the cannula is held at the center of the air bubble. Without exiting the anterior chamber, the cannula is then slowly moved toward the edge of the transplant, positioned underneath the transplant, and again carefully moved toward the pupillary area. At the pupillary border, a small air bubble is injected underneath the DMEK graft to lift the transplant upward toward the recipient cornea. Then the air bubble is slowly enlarged while the edges of the transplant are carefully observed in order to guard against the creation of peripheral inward folds that can undermine graft adherence. If these folds occur, they can be flattened out with a bubble-bumping maneuver—gentle taps of the cannula on the outer corneal surface overlying the fold—to create a flow of aqueous to make the remnant folds disappear (Figure 5).
Once the DMEK graft is completely unfolded, the anterior chamber is filled with air to position the transplant onto the recipient posterior stroma for 60 minutes at approximately 20 mm Hg. Thereafter, a partial air-saline exchange may be performed to leave the eye pressurized with a 30% (in phakic eyes) or 50% (in pseudophakic eyes) air fill in the anterior chamber.
CONCLUSION
With the technique described, 95% of patients can achieve a BCVA of 0.5 (Snellen decimal) or better, and 75% can reach 0.8 or better within 6 months after surgery.1 As with other endothelial keratoplasty techniques, DMEK can be associated with a drop in endothelial cell density in the early postoperative period due to excessive intraoperative manipulation, although this loss can be minimized with the no-touch technique described here.1
Globally—especially in regions where resource shortages or costs are particular concerns—DMEK can have additional advantages, as the operation can be performed in virtually any clinical setting without requiring the use of specialized or expensive equipment for graft creation or the surgery itself. Moreover, the anterior stroma left over from creating a DMEK graft may be reused in anterior lamellar surgery for another patient.5
We believe that DMEK will become a preferred treatment method for corneal endothelial disorders. n
1. Rodríguez-Calvo-de-Mora M, Quilendrino R, Ham L, et al. Clinical outcome of 500 consecutive cases undergoing Descemet’s membrane endothelial keratoplasty. Ophthalmology. 2015;122:464-470.
2. Dapena I, Moutsouris K, Droutsas K, et al. Standardized “no-touch” technique for Descemet membrane endothelial keratoplasty: Arch Ophthalmol. 2011;129:88-94.
3. Melles GR, Dapena I. “No-touch” DMEK surgical technique. In: How to Get Started with Standardized “No-Touch” Descemet Membrane Endothelial Keratoplasty (DMEK). Rotterdam: Netherlands Institute for Innovative Oculate Surgery; 2014: 57-72.
4. Dapena I, Ham L, Moutsouris K, Melles GR. Incidence of recipient Descemet membrane remnants at the donor-to-stromal interface after descemetorhexis in endothelial keratoplasty. Br J Ophthalmol. 2010;94:1689-1690.
5. Groeneveld-van Beek EA, Lie JT, Van der Wees J, Bruinsma M, Melles GR. Standardized “no-touch” donor tissue preparation for DALK and DMEK: harvesting undamaged anterior and posterior donor transplants from the same donor cornea. Acta Ophthalmol. 2012;91:145-150.
6. Liarakos VS, Dapena I, Ham L, et al. Intraocular graft unfolding techniques in Descemet membrane endothelial keratoplasty. JAMA Ophthalmol. 2013;131:29-35.
Lamis Baydoun, MD, PhD
• Consultant Ophthalmologist and Cornea Surgeon, Netherlands Institute for Innovative Ocular Surgery, Rotterdam, Netherlands
• Cornea Specialist, Melles Cornea Clinic Rotterdam, Netherlands
• Financial disclosure: Consultant (DORC International/Dutch Ophthalmic USA)
Isabel Dapena, MD, PhD
• Consultant Ophthalmologist and Cornea Surgeon, Netherlands Institute for Innovative Ocular Surgery, Rotterdam, Netherlands
• Head of the Medical Department, Melles Cornea Clinic Rotterdam, Netherlands
• Financial disclosure: Consultant (DORC International/Dutch Ophthalmic USA)
Vasilis Liarakos, MD, PhD
• Cornea Specialist, Netherlands Institute for Innovative Ocular Surgery, Rotterdam, Netherlands
• Cornea Specialist, Melles Cornea Clinic Rotterdam, Netherlands
• Financial disclosure: None
Salvatore Luceri, MD
• Cornea Fellow, Netherlands Institute for Innovative Ocular Surgery, Rotterdam, Netherlands
• Cornea Fellow, Melles Cornea Clinic Rotterdam, Netherlands
• Financial disclosure: None
Gerrit R.J. Melles, MD, PhD
• Cornea Specialist and Director, Netherlands Institute for Innovative Ocular Surgery, Rotterdam, Netherlands
• Director, Melles Cornea Clinic Rotterdam, Netherlands
• Director, Amnitrans EyeBank Rotterdam, Netherlands
• research@niios.com
• Financial disclosure: Consultant (DORC International/Dutch Ophthalmic USA, SurgiCube International)
Jack Parker, MD
• Research Fellow, Netherlands Institute for Innovative Ocular Surgery, Rotterdam, Netherlands
• Research Fellow, Melles Cornea Clinic Rotterdam, Netherlands
• Financial disclosure: None
Jorge Peraza-Nieves, MD
• Cornea Fellow, Netherlands Institute for Innovative Ocular Surgery, Rotterdam, Netherlands
• Cornea Fellow, Melles Cornea Clinic Rotterdam, Netherlands
• Financial disclosure: None