

The introduction of femtosecond lasers to perform crucial steps of cataract surgery has created renewed interest in the potential value of the capsular opening.1,2 Compared with a manually created capsulorrhexis, laser anterior capsulotomy can more closely and consistently approximate the intended surgical opening in terms of size, shape, centration, and regularity.3,4 The enhanced precision and accuracy of a laser anterior capsulotomy has made creating a capsular opening an easier task for surgeons and raised the intriguing potential of using the laser to improve surgical results.
At a Glance
• The enhanced precision and accuracy of laser anterior capsulotomy has made the creation of a capsular opening an easier task for surgeons; however, at the microstructural level, there are concerns about the safety of using the laser to create a capsulotomy.
• Laser settings, differences in imaging systems among the available femtosecond platforms, and differences in surgeons’ preferred treatment algorithms can influence the way a laser anterior capsulotomy is constructed and affect capsular edge strength; this may account for differences in anterior capsular tear rates reported with laser anterior capsulotomy.
As Richard Packard, MD, FRCS, FRCOphth, states in his opening article to this cover focus, the capsulotomy has evolved beyond being a mere opening through which the cataract is removed to become a controlled structural aperture that can influence effective lens position and refractive outcomes.5-7
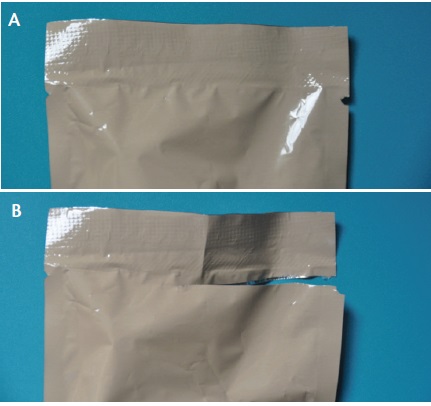
Figure 1. Photograph of serrated edge on plastic packaging (A). Photograph of tear extending from serrated spot on packaging (B). These photographs help depict that tears are harder to create outside the serrated spot.
RISK OF TEARS
Recent conflicting clinical reports on anterior capsular tear rates have raised concern about the risk-benefit profile of laser anterior capsulotomy compared with manual capsulorrhexis. In a large series of 4,000 eyes, Abell and coworkers reported a nine times greater frequency of anterior capsular tears when a laser was used to create the capsulotomy (1.84% vs 0.22%, laser vs manual).8 However, the same study also found no significant differences in posterior capsular tear rates between the two groups. It appears that the learning curve has an effect on anterior capsular tear rates with regard to anterior laser capsulotomy. Chang and coworkers reported a 5.3% anterior capsular tear rate in their early experience with laser capsulotomy creation,9 and Roberts and colleagues reported no differences in anterior capsular tear rates between manual capsulorrhexis and laser anterior capsulotomy after an initial learning curve was overcome.10 After the first 200 eyes, Roberts reported, anterior and posterior capsular tear rates dropped from 4% to 0.3%.
DETERMINING FACTORS IN EDGE STRENGTH
By Harvey Siy Uy, MD
Pulse energy levels. Friedman and coworkers demonstrated that laser anterior capsulotomy edge strength was inversely proportional to laser pulse energy. Scanning electron microscopy (SEM) images of excised capsular buttons produced with a manual capsulorrhexis were smoother than laser anterior capsulotomy button edges, which contained laser-induced microgrooves.1 Sándor and colleagues investigated the effect of different pulse energy levels on capsulotomy strength in porcine eyes by measuring the stretch forces required to rupture the anterior capsule edge. They demonstrated that capsules treated with higher energy levels (10 μJ) required significantly less force to rupture compared with those cut with low or intermediate pulse energy levels (2 and 5 μJ). SEM images revealed that capsule edges were serrated at all energy levels but that additional signs of collagen melting and denaturation were seen with higher energy levels.2 Additionally, Mayer et al demonstrated that cell death along capsule edges was significantly greater with higher pulse energy levels (15 μJ) compared with those cut using lower energy levels (5 μJ). The capsule edges cut using lower pulse energy levels were also smoother and more roundly shaped (see Figure 2 in main article).3
On a slight tangent, our personal experience indicates a lower rate of posterior capsular opacification (PCO) formation following laser anterior capsulotomy compared with manual capsulorrhexis. This suggests the need to study the effect of cell death on lens epithelial cell migration and rates of PCO. It would be interesting to see whether there is a sweet spot in energy pulse levels at which capsular edge strength is retained at sufficient levels while preventing PCO formation.
Capsular diameter. Packer and coworkers hypothesized that that the location and diameter of the capsulotomy may influence edge strength.4 Histologic studies by Barraquer previously demonstrated that anterior capsular thickness ranged from 11 to 13 μm at the anterior pole to 13.5 to 16 μm at the anterior midperiphery to 7 μm at the equator. Maximal capsular thickness appears to be located at a diameter of 4.9 to 5.5 mm. Packer et al, therefore, recommended that the optimal laser anterior capsulotomy diameter in terms of capsular strength should be approximately 5.25 mm (see Figure 3 in main article).
Interface type. Bala and coworkers reported fewer tags and tears and greater homogeneity of capsular edge points when they switched from the presoft fit interface (version 2.16) of the LenSx laser (Alcon) to the soft-fit interface (version 2.20).5
Eye stability. Stability of eye positioning during treatment is likely an important factor. The more eye movement, the greater the chance of laser spots being placed incorrectly and causing uneven capsular edges. Related to this is the speed of treatment: The faster the treatment can be applied, the less likely that patient movement can cause irregularity of the capsular edges.
1. Friedman NJ, Palanker DV, Schuele G, et al. Femtosecond laser capsulotomy. J Cataract Refract Surg. 2011; 37:1189-1198.
2. Sándor GL, Kiss Z, Bocskai ZI, et al. Evaluation of the mechanical properties of the anterior lens capsule following femtosecond laser capsulotomy at different pulse energy settings. J Refract Surg. 2015;31(3):153-157.
3. Mayer WJ, Klaproth OK, Ostovic M, et al. Cell death and ultrastructural morphology of femtosecond laser-assisted anterior capsulotomy. Invest Ophthalmol Vis Sci. 2014;55(2):893-898.
4. Packer M, Teuma EV, Glasser A, Bott S. Defining the ideal femtosecond laser capsulotomy. Br J Ophthalmol. 2015;99(8):1137-1142.
5. Bala C, Xia Y, Meades K. Electron microscopy of laser capsulotomy edge: Interplatform comparison. J Cataract Refract Surg. 2014;40(8):1382-1389.
What may account for these differences in clinical findings? Laser settings, differences in imaging systems among the available femtosecond platforms, and differences in surgeons’ preferred treatment algorithms can all influence the way a laser anterior capsulotomy is constructed. This may, in turn, affect capsular edge strength and account for differences in anterior capsular tear rates.
Do laser anterior capsulotomies have inferior edge strength compared with manual capsulorrhexes? Are they more prone to capsular tears? These are questions that cause concerns among those performing or considering performing laser-assisted cataract surgery (LACS). The rest of this article focuses on structural differences between laser anterior capsulotomy and manual capsulorrhexis and examines factors that may influence the strength of capsulotomies created with the femtosecond laser.
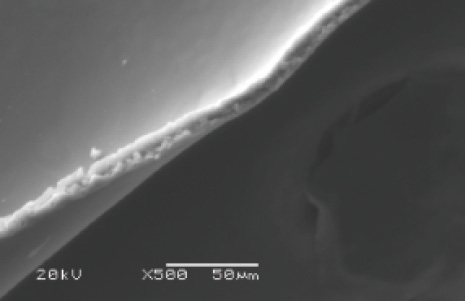
Figure 2. Laser anterior capsulotomy edge cut using low energy level (4 μJ), demonstrating minimal irregularities and approximating the smooth edge of a manual capsulorrhexis.
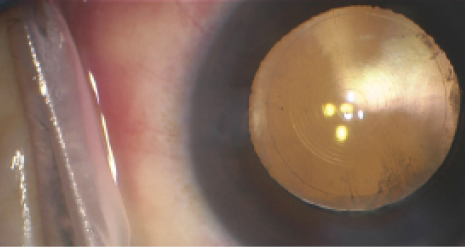
Figure 3. Operating microscope view of multifocal IOL centered behind a 5.25-mm laser anterior capsulotomy.
DIFFERENCES EXAMINED
In terms of gross morphology, the superiority of a laser anterior capsulotomy over a manual capsulorrhexis has been demonstrated in laboratory and clinical studies. Laser-formed capsular buttons undoubtedly outperform those of manual capsulorrhexes in terms of regularity, circularity, and achieving target diameter. At this gross level, the ability of femtosecond lasers to create an ideally sized and shaped opening offers some advantages. Hard, sharp nuclear pieces and the increased number of surgical maneuvers needed to remove them can stress suboptimal capsular openings that are too small, eccentric, or irregularly shaped with the consequence of a capsular tear. Laser anterior capsulotomy minimizes these risks because these capsular openings are consistently of adequate size, circularity, and centration.
It is at the microstructural level where most concerns about the safety of laser anterior capsulotomy arise. Scanning electron microscopy (SEM) studies have demonstrated that the capsular edges of laser anterior capsulotomies are less smooth than manual capsulorrhexis edges. These serrated edges are believed to tear with less stress force than smooth edges. An analogy can be seen in commercial packaging with built-in serrated portions to allow easy opening (Figure 1). Also using SEM, Trivedi and coworkers demonstrated a direct correlation between capsular edge strength and edge smoothness and showed that irregular edges were more prone to anterior tears.11 Al Harthi and coworkers, also using SEM, reported that the edges of laser anterior capsulotomies created with two different laser platforms equally demonstrated marked irregularity, in contrast with the smooth edges of manual capsulorrhexes.
SUMMARY
Several factors have been proposed to influence laser anterior capsulotomy edge strength (see Determining Factors in Edge Strength). Growing experience with laser anterior capsulotomy and improvements in technologies have led to greater understanding of the impact of treatment parameters on the microstructure of laser anterior capsulotomy and resulting capsular strength (Figure 2). Optimization of pulse energy levels, shot spacing, and speed of treatment should lead to improvements in the safety of LACS, better effective lens positioning (Figure 3), and possibly lower PCO rates. n
1. Nagy Z, Takacs A, Filkorn T, Sarayba M. Initial clinical evaluation of an intraocular femtosecond laser in cataract surgery.
J Refract Surg. 2009;25:1053-1060.
2. Palanker DV, Blumenkranz MS, Andersen D, et al. Femtosecond laser-assisted cataract surgery with integrated optical coherence tomography. Sci Transl Med. 2010; 2(58):58ra85.
3. Reddy KP, Kandulla J, Auffarth GU. Effectiveness and safety of femtosecond laser–assisted lens fragmentation and anterior capsulotomy versus the manual technique in cataract surgery. J Cataract Refract Surg. 2013;39(9):1297-1306.
4. Tackman RN, Villar Kuri J, Nichamin LD, Edwards K. Anterior capsulotomy with an ultrashort-pulse laser. J Cataract Refract Surg. 2011;37(5):819-824.
5. Filkorn T, Kovacs I, Takacs A, Horvath E, Knorz MC, Nagy ZZ. Comparison of IOL power calculation and refractive outcome after laser refractive cataract surgery with a femtosecond laser versus conventional phacoemulsification. J Refract Surg. 2012:28:540-544.
6. Hill WE, Uy HS, Edwards K. Refractive outcomes in large cohort of laser refractive cataract surgeries. Paper presented at: American Society of Cataract and Refractive Surgery Annual Meeting. Chicago, April 2012.
7. Kranitz K, Mihaitz K, Sandor GL, Knorz MC, Nagy ZZ. Intraocular lens tilt and decentration measured by Scheimpflug camera following manual or femtosecond laser-created continuous circular capsulotomy. J Refract Surg. 2012:28(4):259-263.
8. Abell RG, Darian-Smith E, Kan JB, Allen PL, Ewe SY, Vote BJ. Femtosecond laser-assisted cataract surgery versus standard phacoemulsification cataract surgery: outcomes and safety in more than 4000 cases at a single center. J Cataract Refract Surg. 2015;41(1):47-52.
9. Chang JS, Chen IN, Chan WM, Ng JC, Chan VK, Law AK. Initial evaluation of a femtosecond laser system in cataract surgery. J Cataract Refract Surg. 2014;40(1):29-36.
10. Roberts TV, Lawless M, Bali SJ, Hodge C, Sutton G. Surgical outcomes and safety of femtosecond laser cataract surgery: a prospective study of 1500 consecutive cases. Ophthalmology. 2013;120(2):227-233.
11. Trivedi RH, Wilson ME Jr, Bartholomew LR. Extensibility and scanning electron microscopy evaluation of 5 pediatric anterior capsulotomy techniques in a porcine model. J Cataract Refract Surg. 2006;32(7):1206-1213.
12. Al Harthi K, Al Shahwan S, Al Towerki A, Banerjee PP, Behrens A, Edward DP. Comparison of the anterior capsulotomy edge created by manual capsulorhexis and 2 femtosecond laser platforms: Scanning electron microscopy study. J Cataract Refract Surg. 2014;40(12):2106-2112.
Harvey Siy Uy, MD
• Private practice, Peregrine Eye and Laser Institute, Makati, Philippines
• harveyuy@yahoo.com
• Financial disclosure: Principal investigator (Alcon, Lensar, Novartis)