


Limbal stem cells can be partially or totally depleted, resulting in varying degrees of stem cell deficiency and resulting abnormalities on the ocular surface. These abnormalities, such as corneal neovascularization, scarring, and persistent epithelial defects, can cause symptoms of reduced vision or blindness, chronic ocular irritation, and discomfort.1-3
AT A GLANCE
• Limbal stem cells can be partially or totally depleted, resulting in varying degrees of stem cell deficiency and abnormalities in the ocular surface.
• The etiology of limbal stem cell deficiency varies; the condition can be either inherited or acquired.
• Ocular surface reconstruction and stem cell transplantation for limbal stem cell deficiency require thorough assessment, diagnosis, and planning.
The etiology of limbal stem cell deficiency varies; it can be either inherited, as with aniridia-related keratopathy or ectodermal dysplasia, or acquired, as with Stevens-Johnson syndrome or ocular cicatricial pemphigoid due to thermal or chemical injury or iatrogenic causes in the form of extensive contact lens wear or surgery.4
Standard corneal transplantation—via penetrating or lamellar keratoplasty—is largely unsuccessful in patients with chronic limbal stem cell deficiency (Figure 1). This poor success rate is due to failure to restore the stem cell population and provide limbal barrier function against abnormal conjunctival ingrowth.5
This article describes some of the considerations and choices in treatment of this challenging condition.

A COMPREHENSIVE DIAGNOSIS IS OF UTMOST IMPORTANCE
The diagnosis of limbal stem cell deficiency is made based largely on the natural history of the disease and clinical signs of conjunctivalization of the corneal surface, which is the most specific sign. Other signs, such as superficial vascularization, chronic inflammation, irregular epithelium, and persistent or recurrent epithelial defects, can be also observed in many other corneal diseases without limbal stem cell deficiency.

Figure 1. Failed PKP in a patient with limbal stem cell deficiency.
To confirm conjunctivalization, careful assessment, looking for clinical signs under slit-lamp examination, is crucial (Figure 2). Signs that can be identified include delayed fluorescein staining,6 which reflects poor epithelial barrier function, and the loss of limbal palisades of Vogt.7

Figure 2. Early conjunctivalization of the cornea seen with fluorescein stain (A) and cobalt blue filter (B), where delayed staining can be observed.
Corneal impression cytology staining for goblet cells,8 which are present in the conjunctiva but not the corneal epithelium, and for cytokeratin 19, a marker for conjunctival epithelium, are commonly used. Imaging of the cornea and the limbus, such as with confocal microscopy, can also be of great value as a diagnostic tool.9

A MULTIDISCIPLINARY APPROACH IS NECESSARY IN PREPARATION FOR STEM CELL TRANSPLANTATION
The original disease must be controlled as much as possible. If there is evidence of associated active skin disease, a dermatologist should be involved. In cases of Stevens-Johnson syndrome or mucous membrane pemphigoid, immunosuppression may be necessary.
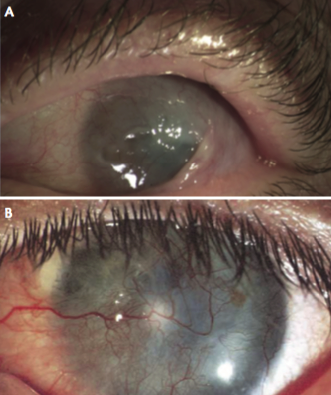
Figure 3. Severe limbal stem cell deficiency with loss of the anatomy of the fornix (A) and corneal vascularization and stromal scarring (B).
Many patients with limbal stem cell deficiency may have coexisting glaucoma. Controlling IOP and eliminating the associated toxicity of antiglaucoma medications on the ocular surface should be an aim of treatment. Glaucoma drainage devices are preferred over trabeculectomy due to the likelihood of conjunctival inflammation and failure with the latter approach.
Any drops to be used must be preservative-free, and unneeded topical medications must be eliminated. Review of systemic medications with the patient’s general physician to remove those that may inhibit tear production is also advisable. Frequent topical steroids will be required preoperatively to prepare the graft site.
Systemic immunosuppression is required in allografts and grafts from living relatives prior to transplantation. General medical review and counseling are also required.

ADNEXAL AND OCULAR SURFACE ANATOMY RESTORATION IS A KEY FACTOR
Stem cell grafts are not likely to be successful unless the lids have good functionality and anatomy. The eyelids must blink completely and regularly, the mucosal surfaces must be wet and nonkeratinized, and the palpebral aperture must be as small as tolerable to minimize evaporative loss. Oculoplastic surgery should be considered to address all of these issues (Figure 3A).
Tear production can be measured with Schirmer testing or meniscometry, and tear osmolarity is also important. In the case of high osmolarity and low tear volume, initial treatment should be with topical steroids and aqueous replacement drops. When these conditions are improved, punctal occlusion and/or partial tarsorrhaphy should be performed. If osmolarity is normal and tear volume is low, minimal steroid drops are needed, but punctal occlusion can be performed immediately.
Severely scarred anterior corneal stroma may not be a good medium for the application of stem cell grafts (Figure 3B). Occasionally, either a preparatory superficial keratectomy and amniotic membrane transplant or anterior lamellar graft is necessary to provide a smooth bed.

DETERMINING THE APPROPRIATE STEM CELL GRAFT METHOD DEPENDS ON MANY FACTORS
For patients in whom stem cell recovery has not been promoted by the measures described in fundamentals No. 1 through 3, a stem cell graft may be required. This decision will depend on whether both eyes are affected, the health of the buccal mucosa, the availability of willing relatives who are human leukocyte antigen matches, and the laboratory facilities available.
For young people of childbearing age, every effort should be made to avoid allografting and the consequent use of immunosuppression, which may interfere with fertility. Allografts from living relatives, autologous corneal grafts, or cultured oral mucosal epithelial transplant may be advantageous.
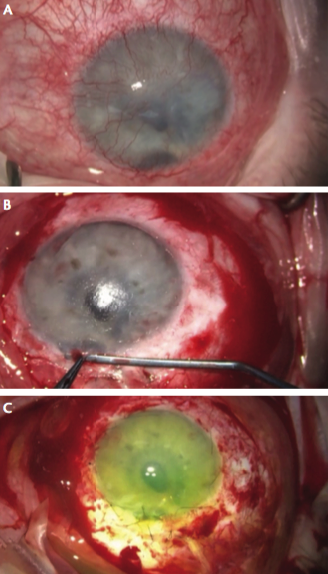
Figure 4. An eye treated with ex vivo stem cell allograft surgery preoperatively (A), during removal of pannus and superficial keratectomy (B), and after placement of a sutured amniotic membrane transplant on top of a stem cell sheet (C).
When the condition is unilateral, a conjunctival limbal autograft may be the method of choice.10 In this procedure, small segments of the limbus from the contralateral eye are transplanted onto the diseased limbus after superficial keratectomy. Depending on the laboratory facilities, the tissue can potentially be expanded ex vivo so that a larger amount of donor tissue can be used. The transplanted limbus then regenerates the ocular surface over time. The advantages of this method are that it is not immunogenic and does not require long-term immunosuppression. However, the possibility of complications in the healthy eye can potentially lead to bilateral blindness.

AN ALLOGRAFT IS THE ONLY CHOICE IN BILATERAL DISEASE
When bilateral disease is present, ex vivo stem cell allograft is the method of choice (Figure 4A).2 Cadaverous limbal tissue is isolated and cultured in growth medium in a specialized laboratory, and a donor stem cell sheet is prepared. The surgical procedure involves conjunctival peritomy, corneal pannus removal, and superficial keratectomy (Figure 4B) or even a corneal transplant if needed, so that a smooth recipient surface is created. The cultured stem cells are then transplanted onto the ocular surface with the sheet of cultured cells, basal-surface down. A fully screened and cryopreserved human amniotic membrane is then sutured on top of the stem cells (Figure 4C).
Postoperatively, intensive topical steroids and autologous plasma eye drops are prescribed. Short-term systemic steroids and prolonged systemic immunosuppression in the form of cyclosporine A or tacrolimus is required. Blood pressure monitoring, serum creatinine, liver function tests, cholesterol, magnesium levels, and cyclosporine/tacrolimus levels must be carried out regularly, and, when necessary, a general physician should be involved.

Figure 5. A patient who underwent ex vivo stem cell allograft surgery combined with PKP at 3 years postoperative.
Cultured oral mucosal epithelial transplant is another available method,11 in which a small biopsy from the buccal mucosa is isolated and cultured in growth medium. The resultant contiguous sheet is transplanted onto the ocular surface after superficial keratectomy. The advantage of this method is that immunosuppression is required only for a short time.
Another method rarely used today is keratolimbal allograft,12 in which cadaverous limbus is directly used to replace diseased limbus. The diseased limbus is resected at the same time that a superficial keratectomy is performed, resulting in restoration of the corneal epithelium. Graft survival rate decreases dramatically over a 2-year period, however, and heavy systemic immune suppression is required.
CONCLUSION
Ocular surface reconstruction and stem cell transplantation for limbal stem cell deficiency require thorough assessment, diagnosis, and planning, with a multidisciplinary approach (Figure 5). Preparation and case selection are key, and various treatment options must be considered.>
1. Schwartz GS, Holland EJ. Classification and staging of ocular surface disease. In: Krachmer JH, Mannis MJ, Holland EJ, eds. Cornea. Philadelphia, PA: Elsevier Mosby; 2011: 1713-1725.
2. Daya SM, Watson A, Sharpe JR, et al. Outcomes and DNA analysis of ex vivo expanded stem cell allograft for ocular surface reconstruction. Ophthalmology. 2005;112(3):470-477.
3. Dua HS, Azuara-Blanco A. Limbal stem cells of the corneal epithelium. Surv Ophthalmol. 2000;44(5):415-425.
4. Cauchi PA, Ang GS, Azuara-Blaco A, Burr JM. A systematic literature review of surgical interventions for limbal stem cell deficiency in humans. Am J Ophthalmol. 2008;146(2):251-259.e2.
5. Holland EJ, Schwartz GS. Changing concepts in the management of severe ocular surface disease over twenty-five years. Cornea. 2000;19(5):688-698.
6. Dua HS, Gomes JAP, Singh A. Corneal epithelial wound healing. Br J Ophthalmol. 1994;78:401-408.
7. Nishida K, Kinoshita S, Ohashi Y, Kuwayana Y, Yamamoto S. Ocular surface abnormalities in aniridia. Am J Ophthalmol. 1995;120:368-375.
8. Puangsricharern V, Tseng SCG. Cytologic evidence ofcorneal diseases with limbal stem cell deficiency. Ophthalmology. 1995;102:1476-1485.
9. Le Q, Wang W, Hong J, et al. An in vivo confocal microscopy and impression cytology analysis of goblet cells in patients with chemical burns. Invest Ophthalmol Vis Sci. 2010;51:1397-1400.
10. Kenyon KR, Tseng SC. Limbal autograft transplantation for ocular surface disorders. Ophthalmology.1989;96(5):709-722.
11. Inatomi T, Nakamura T, Koizumi N, et al. Midterm results on ocular surface reconstruction using cultivated autologous oral mucosal epithelial transplantation. Am J Ophthalmol. 2006;141:267-275.
12. Luca I, Sheraz D. Long-term outcomes of keratolimbal allograft for the treatment of severe ocular surface disorders. Ophthalmology. 2002;109(7):1278-1284.
Damian B. Lake, MBBS, FRCOphth
• Consultant Ophthalmologist, Corneoplastic Unit and Eye Bank, Queen Victoria Hospital, East Grinstead, United Kingdom
• Damian.Lake@qvh.nhs.uk
• Financial disclosure: None
Evripidis Sykakis, MD, MSc, FEBO
• Consultant Ophthalmologist, Eye Day Clinic, Ophthalmological Research Centre, Athens, Greece
• esykakis@gmail.com
• Financial disclosure: None