
Z syndrome is an asymmetric vaulting of a plate-haptic IOL such as the Crystalens (Bausch + Lomb), in which one haptic is bent forward and the other is bent back due to asymmetric forces acting on the lens. In my referral practice, I find that Z syndrome is most likely to occur in smaller eyes (axial length of 22.25 mm or less); however, it may also be more prone to occur in eyes with axial lengths of between 24 and 25 mm that have somewhat steep corneas and thus receive the larger 12-mm AT52 version of the Crystalens used in powers less than 17.00 D, as opposed to the smaller 11.5-mm AT50 platform standard in powers of 17.00 D and greater. The larger the IOL is relative to the capsular bag, the more pressure is placed on the haptics, and the more likely the lens is to vault either posteriorly (U syndrome) or asymmetrically (Z syndrome).
The Z configuration may be promoted by asymmetric capsular contraction due to retained cortex or lens epithelial cells, zonular weakness, wound leakage, eye rubbing, or a large asymmetric capsulorrhexis. Z syndrome may be more likely to occur if the haptics are not properly seated exactly in the equator of the capsular bag, and, although placement of a CTR may reduce risk for the syndrome, it does not completely prevent its occurrence.
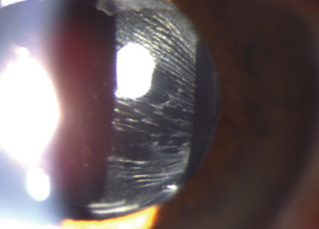
Figure 1. Early recognition of the guitar strings sign in the posterior capsule (stress lines due to early capsular contraction) may enable expeditious treatment and prevention of Z syndrome becoming manifest.
Z syndromes, when they occur, often manifest 3 to 5 weeks after cataract surgery, so it is important to keep an eye out and recognize the signs early, before it has progressed. In many cases, early recognition of the classic guitar strings appearance in the posterior capsule (stress lines due to early capsular contraction) just prior to the onset of a Z can lead to expeditious treatment and prevention of the Z becoming manifest (Figure 1). If this pattern of contraction under one or both haptics is seen before a vault occurs, the process can usually be prevented with Nd:YAG laser treatment applied to the area to break the stress lines.
Once the Z has become established and the lens is tilted, management becomes more difficult. The hallmark of Z syndrome is lenticular astigmatism causing a myopic shift. The lens usually tilts around an axis perpendicular to the haptics, and, thus, minus cylinder on this axis is needed to correct the astigmatism caused by the tilt. The tilt of the lens also induces higher-order aberrations—predominantly coma—so the quality of the patient’s BCVA may suffer in cases of significant tilt.
These situations generally must be corrected. In some cases, judicious application of YAG laser may reverse a significant established Z. If this treatment is unsuccessful, however, then management becomes more complicated; therefore, I generally do not YAG cases of established Z syndrome with loss of BCVA due to coma or if there is more than 2.00 D of induced astigmatism. In these cases, I generally prefer surgical management.
The two approaches to surgical management of Z syndrome are IOL repositioning and IOL exchange. I have had some success freeing up the haptics, rotating the lens 90°, and placing a CTR, but this approach has limited application and success. It cannot be performed if the haptics are too fibrosed in place, as they often are after a few months, and it cannot be done with the toric model of the Crystalens, the Trulign (Bausch + Lomb). Even when this maneuver successfully achieved, there is a significant recurrence rate of about 50%. Videos of this technique can be viewed at https://www.youtube.com/watch?v=AHZKrpPwQKI and https://www.youtube.com/watch?v=zsDGZqnV8pg.
The definitive technique for dealing with Z syndrome causing significant astigmatism and higher-order aberrations is IOL exchange for a nonaccommodating IOL. I generally use a three-piece lens in these cases, but in some cases I use a toric or multifocal IOL as the situation dictates.
It is important to carefully dissect out the plate haptics by stripping the fibrosis off the haptic whiskers so that they can be freed up and removed. In the regions around the plates, there is often significant fibrosis and zonular weakness. If the plates are simply amputated at the hinges, this can lead to migration of these plate remnants into the visual axis over time, which may cause glare or obscured vision, so it is best to remove the whole haptic if possible or amputate most of the haptic if it cannot be extricated from the capsule. I prefer to remove the lens by cutting at the haptic-optic junction (the hinge), removing the optic after cutting it in half, and then removing the plates individually with a haptic-stripping technique. A video of this approach can be viewed at https://www.youtube.com/watch?v=p6HIkH6arFI. If any haptic remnant is left behind, it should be trimmed as short as possible and a CTR should be placed, as in the case shown in the video.

Figure 2. Significant Z syndrome in a 31-year-old patient causing 5.00 D of astigmatism. The patient has been treated with YAG laser unsuccessfully.
If the patient has undergone YAG laser treatment and still has Z syndrome, more advanced surgical techniques will be required, usually involving pars plana vitrectomy, optic capture, and sometimes suturing of the haptics. This is one reason why I am circumspect about doing YAG laser on established Z syndrome. An example of severe Z syndrome after laser cataract surgery and multiple YAG laser treatments can be viewed at https://www.youtube.com/watch?v=-QvC995tN4g, and a video of the repair of the case shown in Figure 2 is at https://www.youtube.com/watch?v=YxMAZmetpfc.
Steven G. Safran, MD
• Private practice in Lawrenceville, New Jersey
• safran12@comcast.net
• Financial disclosure: None