
Getting to Know the Patient
A 72-year-old woman presented with the desire to restore her near vision with a multifocal IOL. Her best friend—my mother—had received multifocal IOLs and spoke highly of them, and this patient wanted to have the same. She was in good health, taking no topical or general medications, and had undergone successful cataract surgery at another center 2 years ago in her left eye. A monofocal hydrophobic blue-light–filtering IOL was implanted in that eye. She complained of residual refractive error for distance and near vision in the pseudophakic eye.
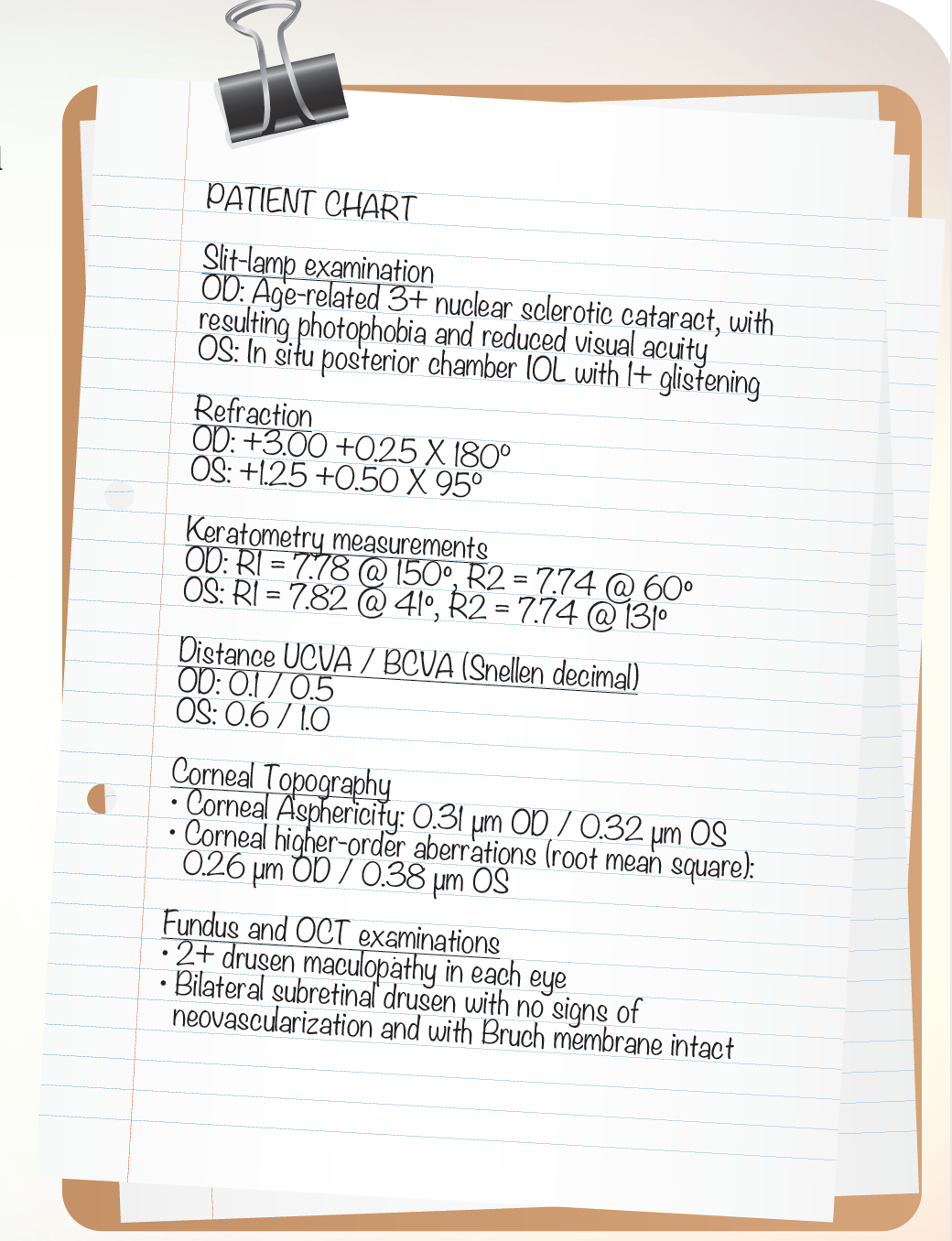
The patient asked for cataract surgery in her right eye with implantation of a multifocal IOL. She also asked about the option of exchanging the monofocal IOL in her left (dominant) eye for a multifocal. Data from her preoperative examination are located in the patient chart to the right.

For a patient who is at risk for age-related macular degeneration (AMD), such as the patient in this case, the choices for IOL selection are limited.1 Based on the findings of our preoperative examination, we felt that we had three options to select from.
Option No. 1: Monofocal blue-light–filtering IOL. In an attempt to avoid multifocal IOL implantation in the patient’s right eye, due to the observed background macular drusen and her risk of developing AMD, implant a monofocal blue-light–filtering IOL, as is present in the patient’s left eye. If this option is selected, a couple of months after surgery, the patient could be offered bioptic correction with femtosecond LASIK, aiming for blended monovision.
Watch it Now
Option No. 2: Multifocal IOLs. Comply with the patient’s request and implant a multifocal IOL in her right eye. In a second surgery, exchange the IOL in the left eye and, at the same time, perform anterior vitrectomy and IOL optic capture.
Option No. 3: Secondary piggyback implant. Implant a secondary piggyback multifocal IOL in the patient’s left eye in order to both correct the residual hyperopia and add near vision correction. Then, in the right eye, perform dual implantation of a blue-light–filtering posterior chamber IOL together with a sulcus-based diffractive multifocal piggyback IOL.2 The dominant eye (left) would receive a near add of 2.50 D at the IOL plane and the nondominant eye (right) a near add of 3.00 D at the IOL plane.3
ELECT TO PIGGYBACK
We decided to choose Option No. 3. With the patient’s background macular drusen, there is a significant chance that she will develop AMD. If so, the diffractive IOL might become disturbing, and the piggyback lens in the right eye could be removed with ease. The already pseudophakic left eye can have the piggyback IOL added and, thus, have both distance and near vision restored.
The posterior chamber IOL chosen for implantation in the patient’s right eye was a 20.50 D hydrophobic Tecnis Optiblue aspheric lens (Abbott Medical Optics). This IOL was chosen because its asphericity value matched that of the patient’s cornea, compensating the eye’s total spherical aberration to almost zero. The blue-light–filtering effect supports protection of the retina from natural and artificial UV light. The hydrophobic material and sharp edge design of the Tecnis Optiblue provide excellent biocompatibility with little chance of capsular shrinkage and posterior capsular opacification in comparison with hydrophilic IOL materials.

Figure 1. The Reverso sulcus multifocal IOL has J-loop, one-size-fits-all haptics.
For the piggyback IOLs, the Reverso multifocal sulcus IOL (Cristalens; Figure 1) was chosen. This lens is not tinted, and it features a diffractive multifocal optic with a range of add powers available. The J-loop one-size-fits-all haptic supports excellent centration and prevents anterior vaulting and iris chafing.
Two other piggyback multifocal IOL models are available, the AddOn (1st Q) and the Sulcoflex (Rayner). In my experience, I have had fewer complications and seen fewer postoperative side effects with the Reverso, so I prefer to use this add-on lens. All piggyback sulcus IOLs are made with hydrophilic materials; no hydrophobic material should be inserted close to the sulcus, or chronic uveitic inflammation could result.
SURGERY
A video of the surgery can be viewed at http://bit.ly/kermani_0616. The first surgery performed was in the patient’s right eye, in order to gauge her acceptance of multifocality. A 2.6-mm clear corneal incision was made temporally. Two sideports of 1.2 mm were also created, and an OVD (ProVisc; Alcon) was injected. Implantation of the Reverso multifocal piggyback IOL (1.00 D sphere with 2.50 D add) was accomplished with a Monarch C cartridge (Alcon). The OVD was removed with irrigation and aspiration. Acetylcholine chloride and cefuroxime were injected at the conclusion of surgery.

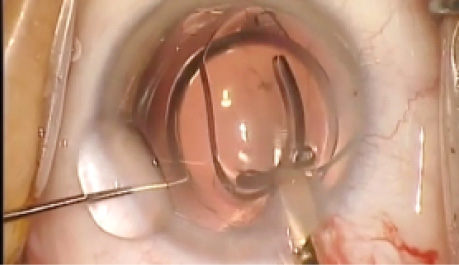
Figure 2. The Reverso lens in situ.
The second surgery, in the patient’s right eye, was performed 4 weeks later. Phacoemulsification and posterior chamber IOL implantation were performed through a 5-mm capsulorrhexis. The posterior chamber IOL, implanted under OVD, was seen to be well positioned. More OVD was instilled, and the Reverso piggyback multifocal IOL was inserted, again using a Monarch C cartridge (Figure 2). The surgery was concluded with irrigation and aspiration of OVD followed by injection of acetylcholine chloride and cefuroxime.
FOLLOW-UP AND LESSONS LEARNED
At 4 weeks postoperative, the patient’s refraction was -0.50 -0.25 X 77° OD and +0.25 -0.50 X 55° OS. Distance UCVA in her right and left eyes was 0.8 and 1.0, respectively; distance BCVA was 1.0 in each eye. Near UCVA in her right and left eyes was 1.0 and 0.8, respectively, and near BCVA was 1.0 in each.
Case Recap
Who
72-year-old woman presenting with one pseudophakic eye and with 2+ drusen maculopathy and subretinal drusen in each eye
What
Requesting a multifocal IOL in her right eye in order to restore near vision and a possible exchange of the monofocal IOL in her left eye for a multifocal
How
Implantation of a secondary piggyback multifocal IOL with a near add of 2.50 D at the IOL plane in the patient’s left eye and dual implantation of a blue-light– filtering posterior chamber IOL together with a sulcus-based diffractive multifocal piggyback IOL with a near add of 3.00 D at the IOL plane in her right
Piggyback IOLs offer a good option to add multifocality when a lens exchange is planned either for medical or refractive reasons. The great value of the piggyback IOL is that reversibility is easily at hand if optical problems or side effects of the diffractive optics turn out to be intolerable to the patient.4 A piggyback multifocal IOL can be implanted secondarily, even years after initial cataract surgery. The secondary IOL can both add near vision and correct a small amount of residual refractive error.
I have not investigated this on a scientific basis, but I have the impression, after implanting hundreds of piggyback multifocal IOLs, that the diffractive optic is better tolerated with a piggyback IOL than with a posterior chamber IOL. The reason may be that, in the sulcus, the optic is much closer to the pupil, and, thus, it is at the cross-point of the optical pathway of the light that enters eye.
1. Schlanitz FG, Baumann B, Kundi M, et al. Drusen volume development over time and its relevance to the course of age-related macular degeneration and lower visual field defects in patients with open-angle glaucoma and high myopia [published online ahead of print April 4, 2016]. Br J Ophthalmol.
2. Gerten G, Kermani O, Schmiedt K, Farvili E, Foerster A, Oberheide U. Dual intraocular lens implantation: Monofocal lens in the bag and additional diffractive multifocal lens in the sulcus. J Cataract Refract Surg. 2009;35:2164-2171.
3. Mastropasqua R, Pedrotti E, Passilongo M, Parisi G, Marchesoni I, Marchini G. Long-term visual function and patient satisfaction after bilateral implantation and combination of two similar multifocal IOLs. J Refract Surg. 2015; 31(5):308-314.
4. Kermani O, Gerten G. Explanatation of multifocal intraocular lenses: frequency, causes and course. Klin Monbl Augenheilkd. [Accepted for publication 2016.]
Omid Kermani, MD
• Executive Director and Medical Director, Augenklinik am Neumarkt, Cologne, Germany
• o.kermani@augenportal.de
• Financial interest: None acknowledged