


We have been performing laser-assisted cataract surgery (LACS) in eyes with traumatic cataracts for several years. The laser has proven to be useful in multiple situations, including lenses with capsular damage (eg, penetrating trauma with capsular rupture or blunt trauma with capsular fibrosis) and with abnormal lens anatomy (eg, resorption).
AT A GLANCE
• In the face of capsular rupture, controlled femtosecond capsulotomy is a distinct advantage.
• Because femtosecond technology is designed to work peripherally, it is well suited for eyes with dense central capsular fibrosis.
• When evaluating a trauma case before deciding on femtosecond laser use, pay close attention to corneal scars and iris damage.
This article describes our use of LACS in these cases and shares some tips for how to make the procedures most effective (see also Surgical Considerations). To watch us perform a procedure using a laser-assisted technique in an eye with trauma to the lens, visit the following link: http://www.mackoolonline.com/december-2012/53-dec12-whitetraumaticfemto.
RUPTURES AND RENTS
In the face of capsular rupture, controlled femtosecond capsulotomy is a distinct advantage. OCT imaging of the capsule can provide direct observation of capsular integrity, and the position and size of the capsulotomy can be adjusted on the fly to avoid irregularities, fibrosis, and rents.

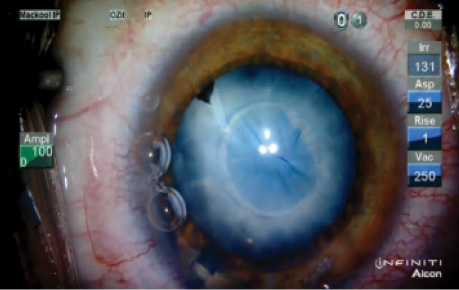
Figure 1. This patient experienced a penetrating ocular injury during which a metallic foreign body passed through both the anterior and posterior capsules. Femtosecond laser treatment of the mature, white, and partially resorbed traumatic cataract was performed.
In the presence of capsular rents, the capsulotomy can be created with a safe margin away from a peripheral rent, or a more central rent can be incorporated within the capsulotomy.
FIBROSIS
When there is dense fibrosis of the capsule, incorporation of the fibrotic areas in or outside of the rhexis with guidance from OCT imaging can be a significant benefit. In cases in which the fibrosis is central, a manual capsulorrhexis would have to be initiated peripherally, involving a higher degree of difficulty, whereas femtosecond technology is designed to work peripherally and is well suited for use in these cases.
The femtosecond laser’s incorporated OCT imaging capability provides a detailed view of the thickness of capsular fibrosis, which can be difficult to assess at the slit lamp. This allows the user to avoid suspect regions of capsule immediately, in real time, by moving or resizing the capsulotomy. In cases in which the fibrosis cannot be avoided, the laser can be adjusted to incorporate the full thickness of the capsule, although manual completion of the rhexis in these areas (eg, with sharp dissection) may still be required.
Watch it Now
LENS RESORPTION
Resorption of the lens in trauma cases is often difficult to assess, as these traumatized lenses are often white and opaque. We have seen excellent OCT penetration of the lens in these cases, and this allows us to assess the lens thickness preoperatively. In several cases, what looked like a white traumatic cataract turned out to be a nearly completely resorbed lens with a residual dense white membranous cataract (Figure 1). In these eyes, sculpting the lens with an ultrasound tip would be unnecessary and could, in fact, damage the posterior capsule.
CORNEAL SCARS
When evaluating a trauma case before deciding on femtosecond laser use, close attention to corneal scars and iris damage is imperative. Traumatic injuries that significantly scar the cornea will limit the coherence of the laser, and, if there is significant corneal scarring, femtosecond laser use may not be feasible.
Trauma patients often present with a limited history, and a faint corneal scar may be the only indication of a previous penetrating injury. Occasionally a small iris defect or transillumination defect in the vicinity of the corneal wound will be the key to diagnosing a previous penetrating trauma.
SURGICAL CONSIDERATIONS
Maximal dilation should be obtained at the preoperative assessment to determine any limitations to femtosecond laser use due to a miotic pupil. Although surgical dilation of the pupil prior to femtosecond laser application has been described, we tend to complete the procedure manually in miotic eyes.
After the preoperative assessment, the standard femtosecond docking procedure is applied and the usual settings utilized. In eyes with capsular damage, we move the capsulotomy margin over suspect areas—if feasible—to image the defects with OCT and to determine the most desirable location for placement of the rhexis. After the zone for laser has been established, we proceed with capsulorrhexis, lens imaging, and lens division.
In dense white traumatic cataracts, laser to the lens is unlikely to be helpful and is therefore bypassed.
CONCLUSION
Femtosecond laser gives the surgeon the ability to perform a controlled capsulotomy and to image the traumatized lens before setting foot in the operating room. In unique and difficult cases, these advantages can make the difference between a successful phaco with an IOL placed in the capsular bag and a less satisfactory result.
Richard J. Mackool Jr, MD
• Assistant Director, Mackool Eye Institute and Laser Center, Astoria, New York
• mackooleye@aol.com
• Financial disclosure: Consultant, Speaker (Alcon)
Richard J. Mackool Sr, MD
• Director, Mackool Eye Institute and Laser Center, Astoria, New York
• mackooleye@aol.com
• Financial disclosure: Consultant, Speaker (Alcon)