



There are many events that, although uncommon, can lead to the need to explant an IOL. Specific situations involving IOLs that can result in the need for explantation include incorrect IOL power calculation, IOL decentration, visual dysphotopsia, and IOL opacification.
AT A GLANCE
• A new explantation device allows any IOL to be removed through a small cataract surgery incision.
• The device consists of a long, narrow loop with a curve that adjusts to the optic of the IOL.
• With two points of support, the device provides a large area of stability for the IOL.
Multiple techniques for explantation that involve either folding or cutting the IOL in the anterior chamber have been described. These methods include full or partial transsection, use of a hinge technique, intraocular refolding, and cutting the IOL into quadrants. There are drawbacks to all of these techniques, and different IOL designs necessitate different methods of removal. In this article, I describe a technique I have devised that can be used to explant any type of IOL. It employs a prototype device constructed for me by ASICO.
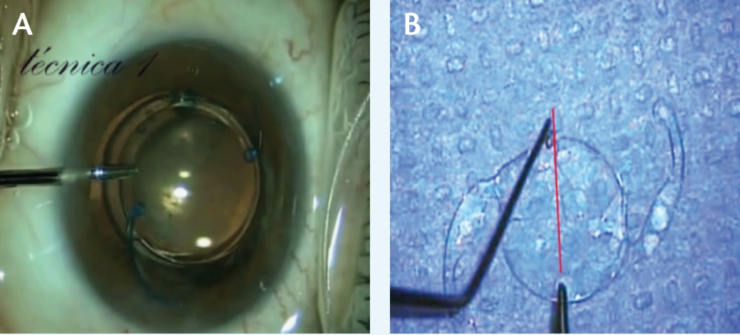
Figure 1. In a commonly used technique for explantation of one-piece IOLs, microforceps grip the IOL while scissors cut it in half for removal (A). If the forceps are not oriented across the diameter of the IOL optic, there is danger of slippage when scissors are used (B).

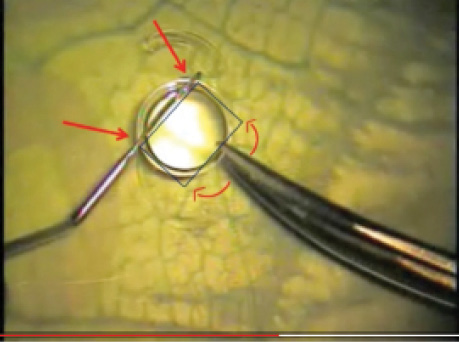
Figure 2. The lens can be twisted from its original orientation (1) when the two points of support are not faced toward the diameter of the optic.
OTHER TECHNIQUES
The technique now perhaps most commonly employed for removal of one-piece IOLs is the use of microforceps to grip the IOL while scissors are used to cut it in half for removal (Figure 1A). The problem with this approach is that it provides only one point of support; if this point and the scissors are not oriented across the diameter of the IOL (Figure 1B), there can be a dangerous shift and slippage of the lens in the eye (Figure 2). The risk of shift is increased, moreover, if the point of support and the scissors form a 90° angle (Figure 3). With the slippage of the lens, if this technique does not permit a one-time cut, the risk of damage to the structures of the angle, the sulcus, and the endothelium is increased. In the example in Figure 4, the circumference of the IOL optic is indicated in yellow. The approximate position of one haptic is indicated in red, suggesting where the opposite haptic is located, causing damage to the sulcus.
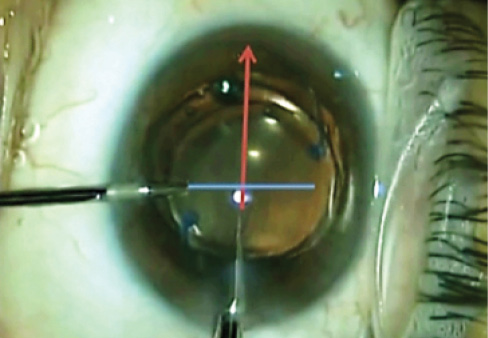
Figure 3. The risk of shift is increased if the point of support and the scissors are at right angles from each other.
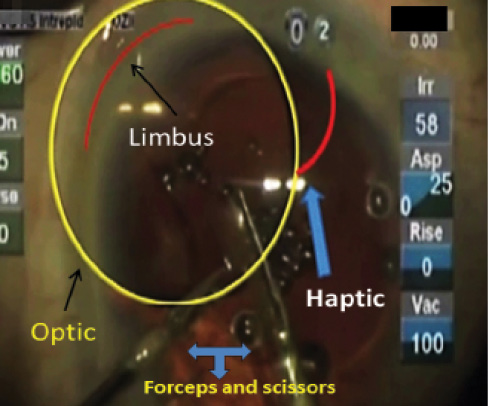
Figure 4. The circumference of the IOL optic is indicated in yellow. The approximate position of one haptic is indicated in red, suggesting where the opposite haptic is located, causing damage to the sulcus.
In another popular technique, commonly used only for three-piece IOLs, one haptic is supported by forceps, and the scissors are introduced to cut the IOL optic. This approach has two problems: (1) there is uncontrolled movement of the lens because it has weak support, and (2) with unconstrained movement of the lens, the optic often becomes vertically oriented.
I have tried other IOL removal techniques that employ devices of larger dimensions. These devices promise to allow cutting or removal of the lens without enlarging the original incisions. I have bought several of these devices, and, in all cases, I have needed to increase the size of the paracentesis and/or main incision. Not only that, but they require pushing the lens against the structures of the angle, causing trauma to the intraocular tissues.
Folding the IOL inside the anterior chamber for removal has also been described. This is difficult to do, with great potential for damage to the incision. The endothelium can also be damaged if the IOL unfolds within the eye, making a sudden movement.
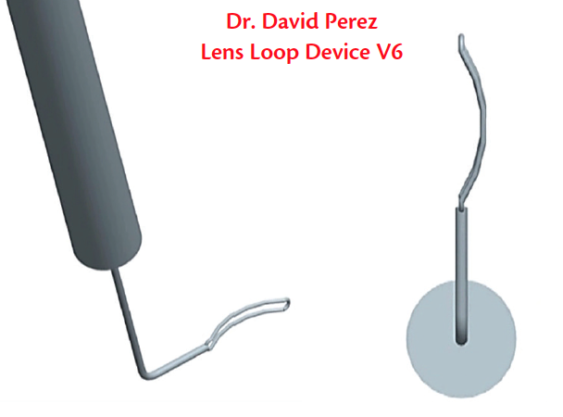
Figure 5. The long, narrow loop of the device (left) can be inserted through a 20-gauge wound. The curve adjusts to the optic of the IOL, providing two points of fixation (right).
REMOVED THROUGH SMALL INCISIONS
The new explantation device allows any IOL to be removed through the small incisions used in modern cataract surgery. It is a long, narrow loop, insertable through a 20-gauge wound, with a curve that adjusts to the optic of the IOL. It works for any lens, whether plate haptic or C-loop (Figure 5).
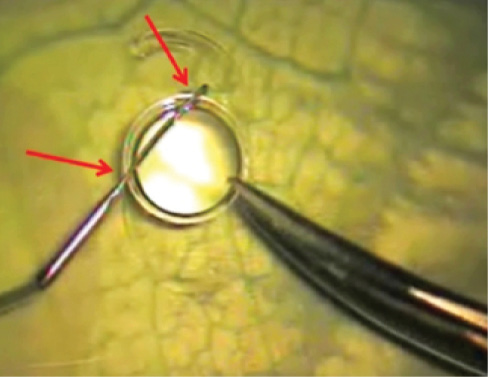
Figure 6. When the IOL is held between the arms of the loop (arrows), it withstands the movements of the scissors without being displaced.
The device offers two points of support, providing a large area of stability for the IOL. When the IOL is held between the arms of the loop, it withstands the movements of the scissors without being displaced (Figure 6). The only other tool needed is Vannas scissors to cut the lens.
The loop will support the IOL and ensure no movement. On the other hand, when necessary, it is easy to disinsert the IOL from the loop, and insert it again. The captured IOL can be positioned as needed, with controlled movements, so that its edge faces the scissors for cutting.
CONCLUSION
This new device is an economical option with a short learning curve. It is valid for use with all types of lenses, can easily be inserted through a 20-gauge paracentesis, and permits controlled management of the IOL during cutting.
Cases in Point
An accompanying video demonstrating three cases with the new device can be viewed at bit.ly/silguero1016. The surgical technique is described here.
First, the IOL is displaced into the anterior chamber, halfway between the endothelium and the posterior capsule. Then, an OVD is injected to protect the endothelium and the posterior capsule. The loop is inserted through a paracentesis and positioned so that a segment of the IOL optic edge is between the two arms of the loop. Vannas scissors, introduced through the main incision, can be used to push the IOL against the loop to place it in the loop, if necessary.
Watch It Now
When this is accomplished, the lens is immobilized and locked in place in the loop, and the loop can be used to manipulate the lens angle with small movements for further control. The IOL can then be cut into manageable pieces with the assurance that it will not move, thus safeguarding the anterior chamber angle, the posterior capsule, and the endothelium.
If long Vannas scissors are used, making long cuts is advised, without removing the scissors until the final cut. If short Vannas scissors are used, the ideal technique is to make small cuts. In either case, it is recommended that the scissors should not be completely closed in successive cuts, so that the scissors always remain on the cutting face. As the IOL is cut, one piece of the portion already cut usually rises a little, and the other moves down. If the scissors are completely closed, or, if the scissors are backed off from the cutting face, then it is difficult to reposition the tip of the scissors in the same place. This is not due to the technique used: It happens with any device inherently, due to the characteristics of the lens material. If the scissors are not completely closed and are not withdrawn from the cutting face, the displacement of the two sides of the lens will not affect the cutting action. The loop will, at all times, maintain IOL stability, allowing a safe and controlled cut.
The first and third cases in the video involve plate-haptic IOLs, which are perhaps the most difficult to explant. The video shows how the loop is introduced through a 20-gauge paracentesis. With pressure from the scissors, a portion of the optic is fitted into the loop, and cutting the IOL is performed in a perfectly controlled manner. The cut can be done clean through or left incomplete, creating a small hinge. Then, with appropriate forceps, the lens portions can be removed.
The second case in the video involves a one-piece IOL with C-loop haptics. The video shows how the Vannas scissors perform the cut as the lens remains stable, without shifting to vertical orientation or causing damage to the intraocular structures.