


Every refractive cataract surgeon wrestles with the question of how to accommodate the occasional need for laser vision correction (LVC) after cataract surgery. Surgeons must determine the best way to price enhancements (in other words, to include them in a refractive package or not), they must convey enhancement policies upfront to patients, and they must choose the most appropriate procedure. This article discusses two ways of approaching enhancements and shares clinical pearls for performing LVC in a refractive cataract surgery practice.
BUFFET VERSUS Á LA CARTE
Buffet pricing. Including LVC enhancements in a laser-assisted cataract surgery (LACS) or premium IOL package is the “all-you-can-eat buffet” approach. Many surgeons find that this method adds value to their refractive packages and simplifies patient counseling, but it can get expensive for the surgeon if his or her enhancement rate is high. The approach may work best for practices with an older patient population. These patients may be highly reassured by the all-inclusive rate. They also may be less likely to pursue enhancements because they are willing to tolerate small amounts of residual refractive error or are simply more conservative about undergoing additional surgery.
AT A GLANCE
• Transparency in explaining the enhancement policy to patients is essential, and it is prudent to discuss with patients the likelihood of needing LVC after cataract surgery.
• Refractive cataract surgeons who own an excimer laser are at an advantage in terms of cost, flexibility, and patient perceptions.
À la carte. A second approach is to charge patients a separate (but reduced) fee for LVC enhancement, making touch-ups an “à la carte” option that patients pay for only when needed. Many surgeons feel this is more fair to patients and that it reinforces the message that surgical services are not free. This method may make it easier to price the premium or LACS package competitively, and it gives the surgeon great discretion in waiving or reducing the enhancement fee in the case of an upset patient or surprise outcome (Figure 1).
SET THE TABLE
Transparency in explaining the enhancement policy to patients is essential, particularly in practices taking the à la carte approach. It is prudent to discuss with patients the likelihood of needing LVC after cataract surgery and the price of the procedure before the initial cataract surgery is performed to avoid bad feelings if a touch-up is needed. When discussing refractive cataract packages, it may be helpful to show the portion of the procedure covered by insurance for a medically necessary cataract, so that patients realize they are getting a discount on refractive surgery because of their cataracts.
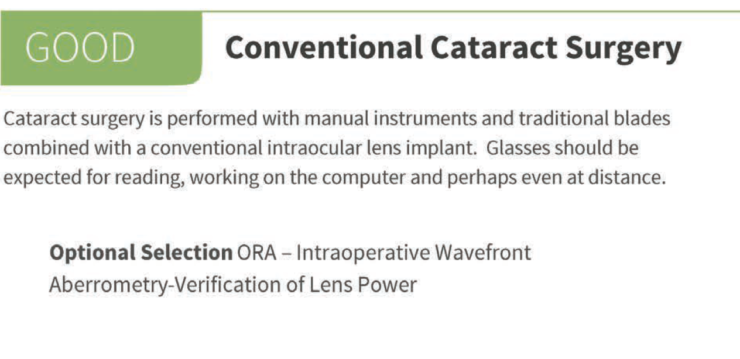
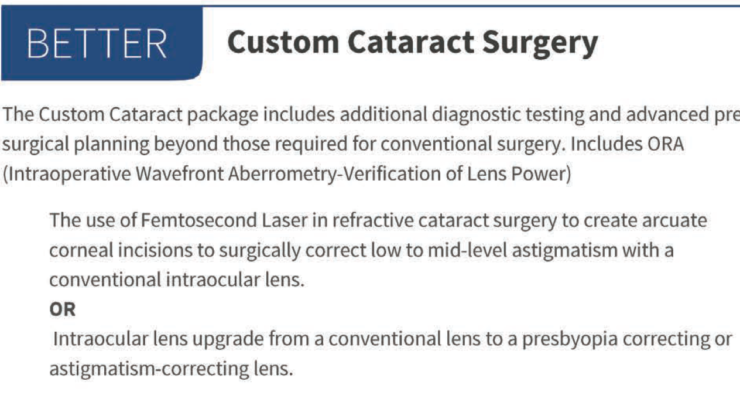
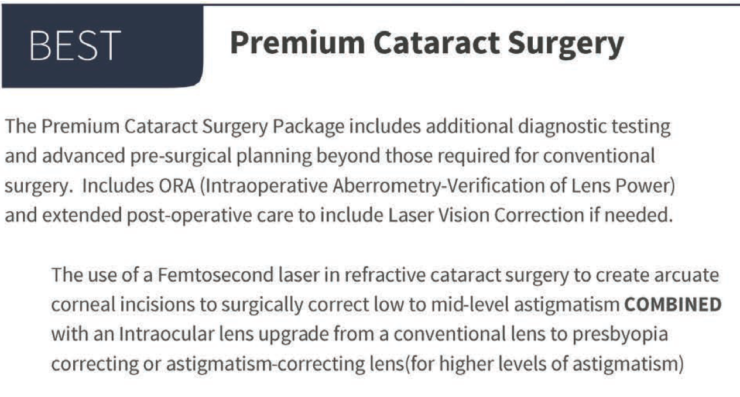
Figure 1. A key difference between the better and best strategies on this pricing menu is the use of both a femtosecond laser and a premium lens in the best package, whereas the better package includes only one of those upgrades. Both the better and best packages include LVC enhancement if needed.
Practices taking the buffet approach may want to market the all-inclusive nature of their packages as a practice differentiator, or they may want to mitigate costs by simply performing enhancements at no charge but not encouraging enhancements by advertising that fact.
ENHANCEMENT TIPS
Refractive cataract surgeons who own an excimer laser and can perform the full range of LVC procedures are at a distinct advantage in terms of cost, flexibility, and patient perceptions. Even if one is referring enhancement patients to a colleague or performing just the occasional surface procedure, it is helpful to understand some common scenarios and considerations for LVC enhancement.
Using the iFs laser, Eva Liang, MD, creates a LASIK flap in an eye with a previous limbal relaxing incision (Top) and then lifts the flap (Bottom).
Tip No. 1: Consider LASIK as the first option. PRK is an effective LVC option and one that cataract surgeons may be more comfortable learning than LASIK, but the delayed healing is a disadvantage, especially in young patients with high expectations. If either is an option, in most cases, there is no reason not to do LASIK.
Tip No. 2: An enhancement should follow suit of the prior refractive surgery. A prior LASIK flap, even an old one, can usually be lifted for an enhancement. If the patient has had prior PRK surgery, any enhancement should also be a surface procedure. A slightly thicker than usual (120 µm) femtosecond laser flap can be created over old RK incisions, as long as there are no more than eight incisions; otherwise, we opt for PRK. LASIK is also possible in the presence of astigmatic keratotomy (AK) incisions performed during LACS. In many cases, the limbal relaxing or AK incisions will be located within the LASIK flap’s diameter, and the iFS femtosecond laser (Abbott) can easily cut through the limbal relaxing or AK incisions.
ICING ON THE CAKE
By Shannon M. Wong, MD
My staff and I have developed a great source of free marketing for our practice: Right after we remove the draping and the patient is sitting up, staffers take a smartphone photo of me with the patient, both of us smiling and giving a thumbs-up (Figure 1). In the photos, my practice’s website is clearly visible on the surgical microscope in the background. My staff emails these photos to patients so they can easily post them to Facebook, the most common social media platform for those aged older than 50 years. A patient might get 50 to 100 “likes” for that postoperative photo—likes that, more often than not, are coming from people in the same age group who are also potential surgical candidates.

Figure 1. Dr. Wong and a happy postoperative patient pose in front of the microscope.
Tip No. 3: Use custom enhancements whenever possible. We prefer custom enhancements whenever possible. Most pseudophakic eyes, including those with presbyopia-correcting or toric IOLs, can be captured and treated with either the WaveScan or iDesign aberrometer (both from Abbott). Taking extra care during refractive cataract surgery to polish the posterior surface of the anterior capsule will help prevent any opacification that might obscure wavefront imaging in the future.
Tip No. 4: Know when to perform the enhancement. Timing may depend on the age and expectations of the patient population. Although many surgeons prefer to wait 3 months after cataract surgery, others perform enhancements as early as 1 month postoperatively to achieve the final visual acuity quicker. It is essential that refractive stability be reached prior to enhancement.
LVC after Crystalens implantation. An Nd:YAG capsulotomy should almost always be performed prior to an LVC enhancement in an eye that has a Crystalens (Bausch + Lomb) to avoid a capsulotomy-related refractive shift after LVC. In these cases, if the patient is mildly myopic, it may also be beneficial to conduct a 1-week contact lens trial to make sure the patient understands the effect of losing near vision.
CONCLUSION
Becoming more comfortable with LVC enhancements will increase your confidence in performing LACS and implanting premium IOLs. We have found it enormously freeing to know that, if the outcome of a refractive cataract surgery procedure is not as expected or desired, the problem can be fixed for the patient. As long as enhancement plans are thought out in advance and clearly communicated to the patient, everyone wins.

