


Case Presentation

An 18-year-old with a history of keratoconous in his right eye was referred to our practice. His left eye was essentially normal with no significant changes. The referring physician told us that, over the past 6 months, he had observed significant progression in corneal steepening in the patient’s right eye, and he wanted to see what we thought.
On examination, the patient’s UDVA was 20/30 OD, but he corrected to 20/20 with a rigid gas permeable (RGP) contact lens. His refraction was -1.25 +1.25 X 85º, and he had been wearing the RGP contact lens occasionally, and, when he did wear it, he saw pretty well. The thinnest pachymetry in this eye was 484 µm, and the maximum keratometry (Kmax) was 55.50 D. Figure 1 shows his topography at the time of his first visit to us: a fairly straightforward presentation of keratoconus.
Our practice was a participating center in the CXL-USA study, and we performed epithelium-on (epi-on) CXL on the patient’s right eye in April 2015 as part of the study’s protocol. As with all cases, I visually inspected the eye at the slit lamp before the UV-A light exposure to make sure that it was saturated with riboflavin. Everything went fine with the treatment.
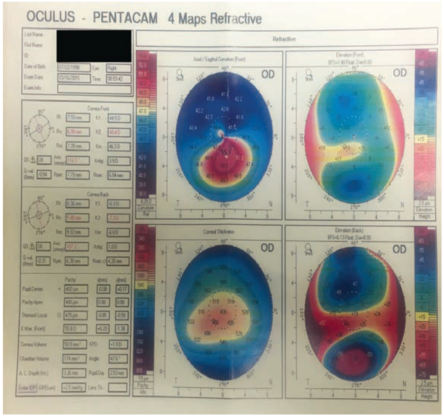
Figure 1. Preoperative topography: fairly straightforward keratoconus.
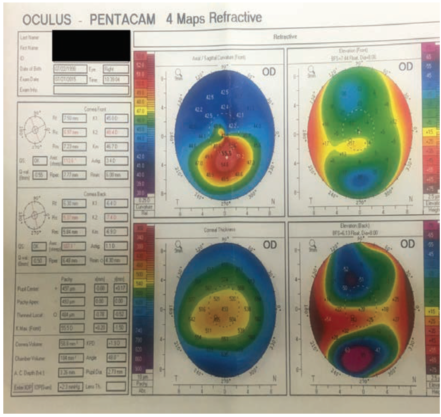
Figure 2. At 3 months postoperative, topography was essentially unchanged.
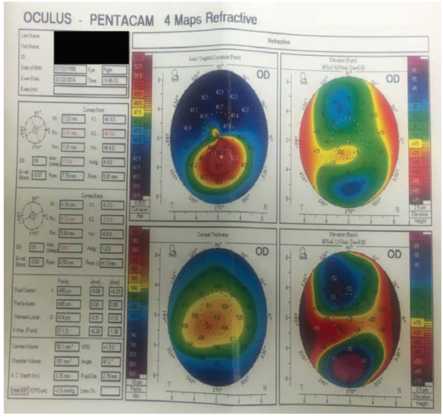
Figure 3. Ten months postoperative: Kmax increased to 57.10 D.
The patient was a college student in Montana, so he had to travel to our center in Spokane, Washington, for follow-up visits. When we saw him in July, about 3 months after his initial treatment, the topography at that visit (Figure 2) was essentially unchanged from the preoperative topography (Figure 1). When a patient does not show the kinds of changes we expect, as was the case here, it is sometimes a cause for concern. Usually we see a bit of change in the postoperative topography, with some flattening in the steep areas and steepening in flatter areas, serving to equalize the corneal curvature.
Because of the travel distance, we did not see the patient again until almost 8 months later, in February 2016. At that visit, the patient said he felt that his vision was good, and there were no notable changes in his vision; UDVA was 20/30, and CDVA was 20/20. However, his Kmax on topography had increased to 57.10 D (Figure 3). Also, his refraction had increased slightly, with a little more cylinder: -1.50 +1.75 X 80º.
Of note, through all of this follow-up, the left eye remained unchanged. At this point, we began to consider retreatment.
Contestants, please comment on several aspects of this case:
- What is your opinion on the decision to re-treat?
- There can be considerable variation in topography maps, even when multiple scans are taken at the same visit. How do you decide when what you are seeing on the map reflects a real clinical change?
- What are your observations regarding the risk of progression in young patients like this one?

Contestant No. 1
I was also a participant in the CXL-USA trial. I agree with you, Mark, regarding the need to verify changes in keratometry. If I think progression is taking place, I acquire several readings with the Pentacam (Oculus) on the same day to see if the progression is real. I also look to see whether the patient has any dry eye issues because of his or her keratoconus. This is an important step, as ocular surface disease can affect topography readings. Has the patient been wearing his or her scleral or RGP lenses, for example? I always want to make sure that I am comparing like with like from visit to visit. All of these things go into making that decision to re-treat.
In general, regarding your third question, our retreatments have been in young males under the age of 22 years, like your patient. We have performed CXL in about 400 eyes at our center, and we have retreated about 10 of them—all in young males with rapid onset and progression.

Contestant No. 2
Mark, when I suspect progression after CXL, I look at the refractive error as well as the topography to evaluate the situation. If the patient’s refraction is getting worse, with increasing astigmatism and/or myopia, this could be a sign that keratoconus is progressing.
In the literature, the retreatment rate for epithelium-off (epi-off) procedures is about 3%.1 At our center, our retreatment rate is 1% for epi-on procedures. So, regardless of the protocol, there will always be a group of patients who will progress. This is why patients must be urged to return for follow-up after CXL, especially young men.
In the CXL-USA study, we are permitted do CXL as an epi-on or as an epi-off treatment, and every patient who has had epi-on CXL has experienced strengthening of their cornea. However, a small percentage of patients do not gain enough corneal strengthening to achieve a complete halt in progression. Everybody in the CXL-USA trial receives the same treatment parameters regardless of their severity of keratoconus, rate of progression, or age. Hopefully in the future we will be able to measure the preoperative level of corneal weakness to customize treatment parameters so that those who require more strengthening can have an extended treatment. For now, when repeat treatments are required, we repeat with the epi-on protocol.

Contestant No. 3
I know that you said there was no disease in the fellow eye, Mark, but it would also be helpful to compare the patient’s two eyes. If progression is evident in both eyes, that makes it more likely that you are seeing true disease progression.
I would certainly agree with the other contestants that young males are the highest-risk group for progression. Additionally, as with all keratoconus patients, it is important to emphasize to these young patients that they should not rub their eyes.
Contestant No. 4
If I thought a patient was progressing despite a first CXL treatment, I would definitely re-treat. In addition to what has been mentioned already as far as clues to establish progression, epithelial mapping, OCT-derived pachymetry maps, and Placido-disc or Cassini (i-Optics) topography may be more objective assessments in the first year after CXL. This is because such methodologies are generally not affected by the CXL-related increase in corneal scatter.
In assessing young potential keratoconus cases, another helpful step is to obtain topography scans for the rest of the family. And, as has been mentioned, some of these patients are avid eye rubbers, even if they do not admit it. One thing that I find helpful, Mark, is to ask whoever comes to the consult with the patient if the patient does indeed rub his or her eyes.
The difficulty with assessing the effect of CXL is that we do not have good metrics for how much we actually achieve. It is always puzzling to look at a patient you treated 2 months ago and see what looks like progression; however, one must keep in mind that it could also be just epithelial hypertrophy or hyperplasia.
Another contestant mentioned obtaining Pentacam maps, but I would argue that this may not be the best way to follow ectasia. There is a change in corneal density after CXL that may throw off Scheimpflug imaging, so perhaps epithelial mapping and Placido-disc mapping are more reliable ways to judge effect.
One of the issues with epi-on treatment—and, I have significant experience with many devices—is that, based on objective metrics (eg, looking at the demarcation line, the cornea, and corneal densitometry with the Pentacam HR), epi-on treatment only achieves similar effect to epi-off treatment when we use UV-A power on the order of 15 J, almost three times the Dresden protocol. I do not see how using 5.4 J of energy with an epi-on treatment will achieve an effect that is even close to that with epi-off; a considerable amount of that energy will be blocked by the riboflavin-soaked epithelium. Again, that is my personal experience, looking at the metrics we have available. Brillouin spectrometry, if it becomes commercially available for ophthalmic use, may tell us more about what we did and did not achieve.
The Resolution
In response to comments from several contestants, I did do multiple topography scans on this patient over a period of about an hour. Because they were fairly consistent, I was confident that there was a change. Also, in response to Contestant No. 4, this patient was an only child, his parents were separated, and his mother accompanied him for visits. If I had been able to, I would have asked his father or any siblings to come in for topography scans to look for clues in family history.
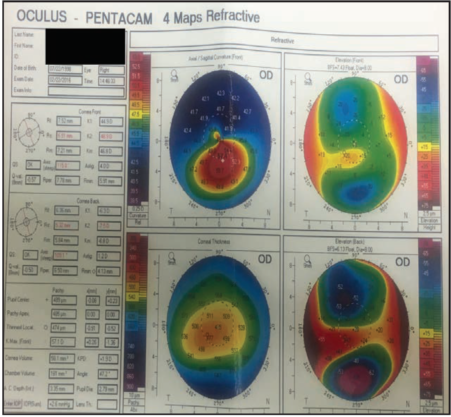
Figure 4. Kmax increased to 57.40 D at 13 months postoperative, indicating slight progression.
So, back to the patient. At the February 2016 visit, I wanted to re-treat, but the patient was unable to undergo treatment at that time because of school requirements. I told him to come back as soon as he could for retreatment. When he returned in May 2016, the patient noted that his vision seemed less clear to him subjectively. His UDVA was slightly worse, at 20/30-2, and his CDVA was unchanged. His Kmax had increased to 57.40 D (Figure 4), indicating that the keratoconus was not progressing rapidly, but it was progressing. I re-treated him at that visit, and, since then, the patient has done well. He has not been back for a recheck of his topography.
I have treated more than 300 keratoconus eyes with CXL, and I have had to re-treat seven of these to date. Of those, four have been cases like the one presented here: young men who had rapidly progressing keratoconus at the time of their treatment and then progressed after CXL. It seems, from the comments of the contestants, that we need to be especially vigilant with follow-up in this population, and we must re-treat when we see evidence of progression after a primary CXL treatment.
1. Antoun J, Slim E, el Hachem R, et al. Rate of corneal collagen crosslinking redo in private practice: Risk factors and safety. J Ophthalmol. 2015. doi:10.1155/2015/690961.
AND THE WINNER IS...
All four contestants made important points, but my choice for the best response is Contestant No. 4 because of his mention of the need to look at the entire family in patients with keratoconus and because of his discussion of epi-on and epi-off treatments.
Educating patients on the familial nature of the disease is significantly important but often overlooked. Also, after being involved in CXL for several years, it is my feeling that there is a place for both epi-on and epi-off treatments in the management of keratoconus patients. We may eventually find that epioff is needed in certain subsets of patients and epi-on in others.
GET TO KNOW THE CONTESTANTS

Contestant No. 1
Audrey R. Talley Rostov, MD
• Partner, Director of Cornea, Cataract and Refractive Surgery, Northwest Eye Surgeons, Seattle, Washington
• Global Medical Director, SightLife, Seattle, Washington
• ATalleyRostov@nweyes.com
• Financial disclosure: None acknowledged

Contestant No. 2
William B. Trattler, MD
• Director of Cornea, Center for Excellence in Eye Care, Miami
• wtrattler@earthlink.net; Twitter @wtrattler
• Financial disclosure: Investor (CXL Ophthalmics)

Contestant No. 3
Rajesh K. Rajpal, MD
• Founder, See Clearly Vision, Virginia and Maryland
• Clinical Associate Professor, Georgetown University Medical Center, Washington, DC
• rrajpal@seeclearly.com
• Financial disclosure: Consultant (Nicox), Chief Medical Officer (Avedro)

WINNER
Contestant No. 4
A. John Kanellopoulos, MD
• Medical Director, The Laservision.gr Research & Clinical Eye Institute, Athens, Greece
• Clinical Professor of Ophthalmology, NYU Medical School, New York
• Associate Chief Medical Editor, CRST Europe
• ajkmd@mac.com
• Financial disclosure: None acknowledged