


Multifocal IOLs with two foci can improve patients’ UDVA and UNVA after cataract surgery or refractive lens exchange. However, with these lenses, patients often struggle with difficulty in intermediate vision. When VSY Biotechnology introduced the Acriva Reviol Tri-ED (Figure 1) with enhanced depth of focus (EDOF), the lens was said to deliver seamless continuous vision. I was excited to hear this, as it seemed like a promising concept to alleviate the gap in intermediate vision that was common with other lenses I had been implanting.
AT A GLANCE
• The Acriva Reviol Tri-ED IOL promises seamless continuous vision with its trifocal design and EDOF feature.
• The semi-apodized active diffractive trifocal structure of this IOL is designed to reduce unwanted diffraction and to increase optical quality with EDOF vision.
Since August 2014, I have implanted this trifocal diffractive IOL bilaterally in 70 patients. We have documented statistically significant differences between preoperative values and 6-month postoperative results for UDVA, UIVA, and UNVA with this lens. We also found statistically significant decreases in spherical and spherical equivalent values.1,2

Figure 1. The Acriva Reviol Tri-ED.
In a clinical study, the defocus curve of the Acriva Reviol Tri-ED showed a tendency toward flattening (Figure 2), which is different from the typical M shape observed with a bifocal IOL.1,2 As a result, the lens provided patients with perfect visual acuity from near to distance, and contrast sensitivity was in the normal range at 6-month follow-up (Figure 3).1,2
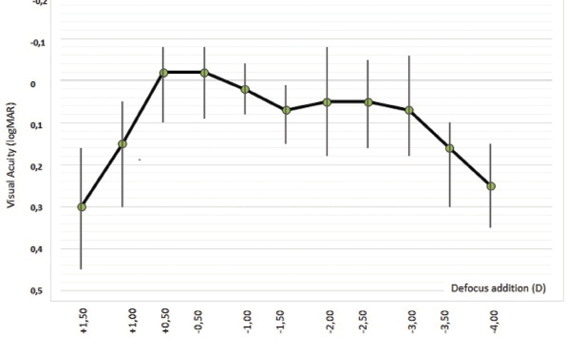
Figure 2. Defocus curve of the Acriva Reviol Tri-ED 6 months after surgery.
In a questionnaire given to all patients in the study at the 6-month postoperative visit, more than 95% reported no difficulty performing vision-related daily activities. Additionally, no patient complained of photic phenomena, and all stated that they were spectacle-free.1,2
A DIFFERENT KIND OF TRIFOCAL
The Acriva Reviol Tri-ED has a one-piece diffractive trifocal EDOF design. The trifocal-EDOF combination is created by changing the height, width, interval, and number of the diffractive rings, with the entire optic diameter covered by 25 rings. There is a real trifocal structure at both the center and periphery, in contrast with other available trifocal IOLs. Furthermore, the EDOF feature provides advantages different from those of other trifocal IOLs. The Reviol Tri-ED can be implanted with the single-use Acrijet Blue 1.8 injector (VSY Biotechnology) through a sub–2-mm incision.3
The Lens: Acriva Reviol Tri-ED
VSY BIOTECHNOLOGY
• Combination of active-diffractive optic and enhanced depth of focus (EDOF) feature
• Trifocal (near add 3.00 D; intermediate add 1.50 D) plus EDOF produces seamless continuous vision
• Diffractive zone design provides higher modulation transfer function values and clear vision at all distances
• Active-diffractive optic provides maximum light transmission to the retina
• Balanced light distribution produces improved contrast sensitivity even in low light conditions
• Fully pupil-independent function
• Plate haptic design with square 360° barrier edge
• Available in a large range of spherical powers (0.00 to 32.00 D in 0.50 D steps)
• Also available in toric configuration

Courtesy of VSY Biotechnology
For more information: http://www.vsybiotechnology.com/en/product/acriva-udreviol-tri-ed-611
The semi-apodized active diffractive trifocal structure of this IOL is designed to reduce unwanted diffraction and to increase optical quality with EDOF vision. Its overall efficiency of global light transmittance is 89.1%, which is higher than that of other trifocal IOLs. Under photopic conditions, this design allocates 40% of light to distance, 30% to intermediate, and 30% to near; under mesopic conditions, 44% of light is allocated to distance, 28% to intermediate, and 28% to near. The lens, therefore, provides adequate visual performance under all light conditions. Furthermore, with an Abbe number of 58—higher than that of other IOLs—it provides better chromatic aberration control.
CASE EXAMPLES
I recommend the Acriva Reviol Tri-ED especially to younger patients who have active lifestyles and who need perfect vision at near, intermediate, and far both day and night. Two case examples will illustrate the benefits of the lens for selected patients.
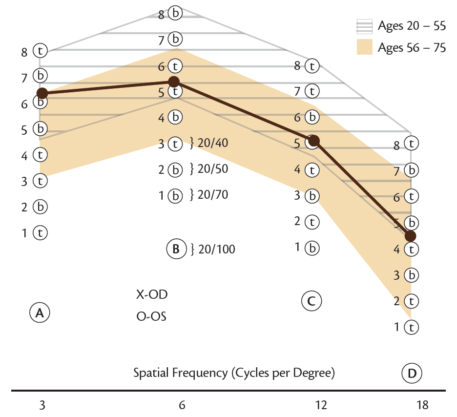
Figure 3. Contrast sensitivity at different spatial frequencies 6 months after surgery.
Case No. 1. A 48-year-old teacher presented with a preoperative refraction of -2.50 D in her right and left eyes. She complained of bad near and intermediate visual acuity and did not want to use glasses for near and far vision. I mentioned trifocal IOLs and recommended implanting the Acriva Reviol Tri-ED bilaterally, especially because of its EDOF feature.
Preoperatively, her UDVA was 0.8 (all measurements logMAR) and CDVA was 0.0 in both eyes. UNVA was 0.4 and CNVA was 0.0 in both eyes. Preoperative UIVA was 1.0 and CIVA was 0.1 in both eyes.
After bilateral implantation of the lens, her UDVA improved to -0.1, UNVA improved to 0.0, and UIVA improved to 0.0 in both eyes. She also reported that her visual acuity was perfect at distance, intermediate, and near and that she was spectacle-independent at all distances. She reported that she had no visual problems, especially when using a computer or reading a book.
Case No. 2. A 65-year-old man who wore glasses came to our clinic complaining of poor visual acuity. During visits to other clinics, he was told that he had a cataract forming and that bilateral cataract surgery was the proper treatment. When he visited our center, he informed us that he wished to be spectacle independent after surgery. Besides being a restaurant manager, the patient has an active lifestyle, including playing tennis and golf and driving. He wanted to see well in mesopic conditions, especially in his restaurant at night.
I recommended implanting the Acriva Reviol Tri-ED because of its optimum light distribution in both daylight and dim light. His preoperative UDVA, UIVA, and UNVA were 0.7, 1.4, and 1.0, respectively, in his right eye and 0.7, 1.3, and 0.9 in his left (all measurements logMAR). He had a nuclear cataract in both eyes.
One month after surgery, UDVA, UIVA, and UNVA improved to 0.0, 0.1, and 0.0, respectively, in both eyes. He was satisfied with his far, intermediate, and near vision and reported having perfect vision in mesopic conditions at his restaurant. Also important to the patient, he has been able to maintain his active lifestyle.
POINTERS AND TIPS
Patient selection is crucial with this lens, as it is with all premium lenses. Patients with any ocular disease (eg, glaucoma, diabetic retinopathy, macular degeneration, corneal disease) and eyes with wide angle kappa may not be the best candidates.
During surgery, it is important to pay attention to properly sizing the capsulorrhexis, thoroughly cleaning the OVD from behind the IOL, and precisely centering the IOL to achieve the best results.
If the reader remembers only one thing about this lens, it should be the promise of seamless continuous vision with its trifocal design and EDOF feature.
1. Torun Acar B, Duman E, Simsek S. Clinical outcomes of a new diffractive trifocal intraocular lens with enhanced depth of focus (EDOF). BMC Ophthalmol. 2016;16(1):208.
2. Acar BT, Duman E, Simsek S. Clinical outcomes of a new trifocal intraocular lens: Reviol tri-ED. Paper presented at: European Society of Cataract and Refractive Surgeons annual meeting; September 5-9, 2015; Barcelona, Spain.
3. Acriva Reviol Tri-ED IOL [product brochure]. VSY Biotechnology. http://www.vsybiotechnology.com/media/2016/08/Reviol_Tri-ED.pdf?v=0.0.1. Accessed December 15, 2016.
