




Short and long eyes are thought to carry increased risk for complications in cataract surgery. Therefore, one may need to adapt the surgical techniques employed for phacoemulsification in these eyes due to their special anatomies.
The main issue in high myopia (-15.00 to -30.00 D) is the high incidence of retinal detachment, which is around 8% within 3 years of phacoemulsification in myopic eyes, compared with 0.4% to 1.2% in the general population.1,2 With increasing axial length, there is an almost linear increase in the incidence of pseudophakic retinal detachment.3
AT A GLANCE
• In high myopia, with increasing axial length there is an almost linear increase in the incidence of pseudophakic retinal detachment.
• Patients with high hyperopia have shorter axial lengths, often associated with a shallow anterior chamber, which makes phacoemulsification more difficult.
• With meticulous preoperative planning and proper intraoperative techniques, cataract surgery can be successful in challenging cases of extreme ametropia.
Thus, for patients seeking refractive surgical correction, surgeons should advise patients to keep their natural lenses if no functional or morphologic changes have occurred. We prefer to implant phakic IOLs, rather than undertake refractive lens exchange (RLE), in myopic patients aged 50 to 60 years who have clear lenses and contact lens intolerance. Nonetheless, in a study we conducted in 107 patients (190 eyes) who had undergone RLE with posterior chamber IOL implantation, the rate of retinal detachment was lower than expected at 2.1% within 3 years after surgery.4
Patients with high hyperopia have shorter axial lengths, often associated with a shallow anterior chamber. This makes phacoemulsification more difficult and increases the incidence of complications, as completing the capsulorrhexis and atraumatically removing the nucleus can be challenging. In these cases, we must act before the cataract progresses too much in order to avoid additional risk factors. Phacoemulsification can also be helpful in short eyes for reduction of high IOP due to angle closure.
This article presents tips for every step of phacoemulsification in the setting of extreme ametropia.

SURGICAL PLANNING, ANESTHESIA, AND INCISION CREATION
Amblyopia is more common in eyes with extreme ametropia than in normal eyes, and reasonable patient expectations should be set prior to surgery. The refractive effect of lensectomy should be considered, and patients with high ametropia and unilateral cataract should be properly counseled that postoperative anisometropia may necessitate surgery in the short term in their other eye.
Topical or peribulbar anesthesia may be used in eyes with extreme myopia or hyperopia. We avoid retrobulbar anesthesia due to higher risk of perforation in myopic eyes (thin sclera and posterior staphyloma) and of high positive pressure in hyperopic eyes that may further narrow the anterior chamber.
We find intravenous mannitol (20%, 1–2 mL/kg) useful in short eyes because it helps decompress the vitreous body, providing a 30% reduction in IOP and posterior displacement of the iris diaphragm. Intravenous mannitol should be given 30 minutes before the main incision is created, as the maximum effect is obtained 45 minutes after administration.
In eyes with high ametropia, it is key to perform meticulous wound construction and create an incision that provides a stable anterior segment. We prefer to place the incision superiorly; however, if the patient has a deep-set orbit, as is common in hyperopic eyes, we instead create the incision temporally and far from the limbus to avoid iris extrusion.
For patients with extreme myopia undergoing implantation of a rigid PMMA IOL, we create two incisions at different levels:
- A 2.2-mm trapezoidal clear corneal incision through which we perform phacoemulsification; and
- A 6-mm valve-type scleral incision through which we introduce the IOL (Figure 1).
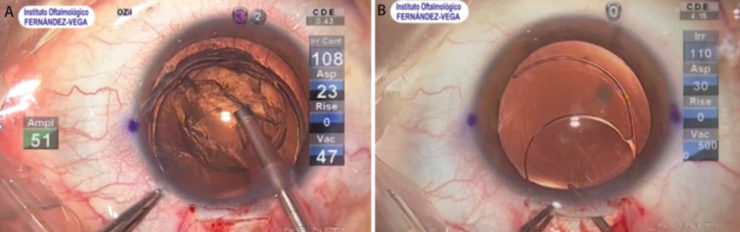
Figure 1. Two incisions are created at different levels in a highly myopic patient undergoing PMMA IOL implantation. A clear corneal incision is used for phacoemulsification (A), and a wider scleral tunnel is used for IOL implantation (B).

THE CAPSULORRHEXIS
Myopic eyes. In myopic eyes, the capsulorrhexis must be big enough to avoid capsular phimosis, which can cover the edge of the IOL optic. A larger capsulorrhexis also facilitates subsequent exploration of the peripheral retina in these long eyes that are at risk of retinal detachment.
Hyperopic eyes. In hyperopic eyes, the capsulorrhexis is prone to tear toward the periphery. Thus, it is important to pay close attention and to refill the anterior chamber with OVD as necessary or to employ the soft-shell technique. Femtosecond laser capsulotomy creation can be helpful in these cases, especially in eyes with an anterior chamber depth of less than 2 to 2.5 mm (Figure 2).
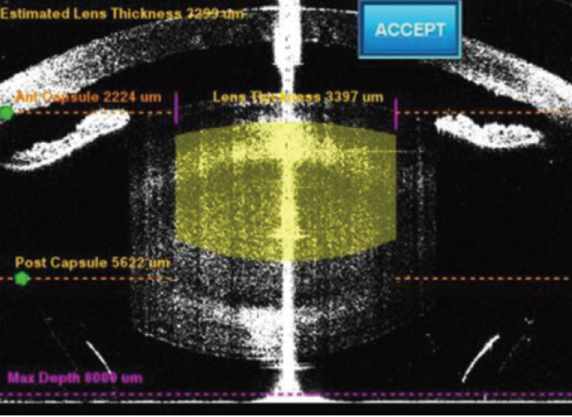
Figure 2. Planning for laser-assisted cataract surgery, to be performed with the LenSx Laser (Alcon), in an eye with an extremely shallow anterior chamber.

PHACOEMULSIFICATION
Myopic eyes. Highly myopic eyes tend to have deep anterior chambers, often accompanied by weak zonules, thin posterior capsules, and a partially liquefied vitreous. Therefore, one’s phaco parameters must be lowered in order to avoid fluctuations in the posterior capsule. Despite this caution, lens-iris diaphragm retropulsion syndrome (deep anterior chamber, mydriasis, and concave iris) may occur due to a reverse pupillary block, producing pain, miosis, and a higher risk of posterior capsular rupture. To avoid this, iris retractors or a second instrument can be put in place to prevent contact between the iris and lens capsule.
Hyperopic eyes. Hyperopic eyes have a propensity for poor dilation and iris prolapse. Raising the infusion bottle height can help to maintain an adequately formed anterior chamber. Phaco energy and lens fragments must be directed away from the endothelium, and the posterior capsule should be protected from contact with the phaco tip by use of a second instrument. Cohesive OVDs do a better job of creating and maintaining space in these eyes compared with dispersive OVDs; strongly cohesive OVDs tend to be the most effective. In rare cases, if the anterior segment remains excessively shallow, a limited pars plana anterior vitrectomy can be performed to reduce volume in the vitreous cavity.
All ametropic eyes. In all cases of high ametropia, we implant a capsular tension ring to provide stability to the capsular bag, facilitate anterior and posterior capsule polishing, provide centration of the IOL, and decrease and distribute zonular tension. The ring also facilitates future surgery in the event of IOL dislocation or the need for IOL exchange due to refractive surprise, which is more likely in extreme ametropia.5

IOL SELECTION
Myopic eyes. Myopes are used to having good near vision when they remove their glasses. In these eyes, therefore, we must try to maintain good near vision after cataract surgery. If we implant a monofocal IOL, our target refraction for distance is -1.50 D. We do not implant trifocal IOLs in patients with axial lengths greater than 30 mm or in eyes in which there is a staphyloma that involves the macula.
Hyperopic eyes. In small hyperopic eyes, we prefer IOLs with flexible C-loop haptics to avoid ovalization of the anterior capsule with displacement of the optic, as can be seen with plate-haptic IOLs (Figure 3). If the optic is very thick because of high refractive power, the incision may have to be enlarged to avoid inducing damage during insertion. The CT Xtreme D (Carl Zeiss Meditec), a customizable one-piece foldable monofocal aspheric IOL, available in refractive powers from 45.00 to 60.00 D, is one available option for short eyes.6 When we decide to implant a trifocal IOL, we ensure that the patient is aware of the loss of image magnification.
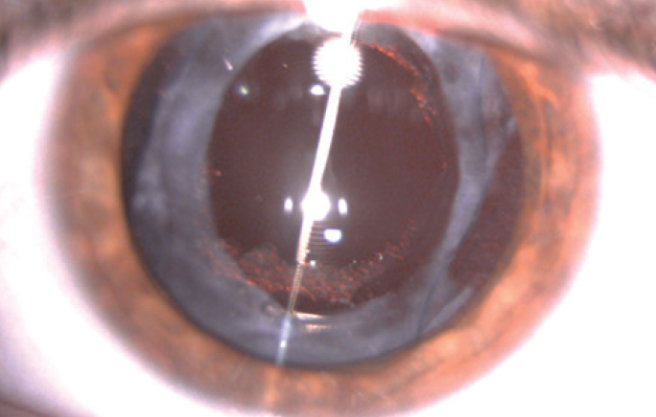
Figure 3. Anterior capsule ovalization in an eye with a plate-haptic IOL.

BIOMETRY
Refractive outcomes are less predictable in cases of extreme ametropia than in normal eyes due to inaccuracies in measurement of biometry and because the classical IOL power calculation formulas assume that long eyes have a large anterior segment and short eyes have a small anterior segment. This assumption is inaccurate.
Myopic eyes. If the surgeon’s regular IOL constant and standard power formulas are used in myopic eyes, a hyperopic shift results, which is greater the longer the eye.7
In designing his power calculation formula, Haigis considered the constants that were used in older formulas and proposed that IOL geometry must change at the transition from plus to minus powers; therefore, a corresponding change should be applied to the IOL constants. If no allowance is made for this effect, refractive errors increasing with axial length will be associated with minus-power IOLs.8 If the constant is not changed, we must under-correct9 or transform the axial length obtained with biometry by use of the Wang formula.10
Hyperopic eyes. Accurate biometry is crucial in short eyes because small errors in axial length and effective lens position have a large effect on refractive outcomes. Whereas an axial length that is wrong by 1 mm in a normal eye may induce 3.00 D of error, in a short eye the error may be as high as 5.00 D because of the high refractive power of the IOL.9
For this reason, we must be careful when obtaining measurements in short eyes and use optical or immersion biometry whenever possible. It is also advisable to use newer formulas, such as the Holladay 2, Haigis, Hoffer Q, Olsen, and Barrett, which incorporate additional data such as the white-to-white measurement, refraction, and anterior chamber depth to produce more accurate results.11
CONCLUSION
With careful preoperative planning and the appropriate intraoperative techniques, cataract surgery can be successful in these challenging cases of extreme ametropia. If trouble presents, exercise patience, introduce OVD, and think carefully.
1. Ripandelli G, Scassa C, Parisi V, Gazzaniga D, D’Amico DJ, Stirpe M. Cataract surgery as a risk factor for retinal detachment in very highly myopic eyes. Ophthalmology. 2003;110(12):2355-2361.
2. Boberg-Ans G, Villumsen J, Henning V. Retinal detachment after phacoemulsification cataract extraction. J Cataract Refract Surg. 2003;29(7):1333-1338.
3. Ogawa A, Tanaka M. The relationship between refractive errors and retinal detachment--analysis of 1,166 retinal detachment cases. Jpn J Ophthalmol. 1988;32(3):310-315.
4. Fernandez-Vega L, Alfonso JF, Villacampa T. Clear lens extraction for the correction of high myopia. Ophthalmology. 2003;110(12):2349-2354.
5. Schild AM, Rosentreter A, Hellmich M, Lappas A, Dinslage S, Dietlein TS. Effect of a capsular tension ring on refractive outcomes in eyes with high myopia. J Cataract Refract Surg. 2010;36(12):2087-2093.
6. Singh H, Wang JC, Desjardins DC, Baig K, Gagne S, Ahmed II. Refractive outcomes in nanophthalmic eyes after phacoemulsification and implantation of a high-refractive-power foldable intraocular lens. J Cataract Refract Surg. 2015;41(11):2394-2402.
7. Zaldivar R, Shultz MC, Davidorf JM, Holladay JT. Intraocular lens power calculations in patients with extreme myopia. J Cataract Refract Surg. 2000;26(5):668-674.
8. Haigis W. Intraocular lens calculation in extreme myopia. J Cataract Refract Surg. 2009;35(5):906-911.
9. Aramberri J. IOL power calculation. SECOIR Diagnosis Guide. 2013. Available at: http://secoir.org/wp-content/uploads/sites/5/2015/12/guia-calculo_potencia.pdf. Accessed April 25, 2017.
10. Wang L, Shirayama M, Ma XJ, Kohnen T, Koch DD. Optimizing intraocular lens power calculations in eyes with axial lengths above 25.0 mm. J Cataract Refract Surg. 2011;37(11):2018-2027.
11. Eom Y, Kang SY, Song JS, Kim YY, Kim HM. Comparison of Hoffer Q and Haigis formulae for intraocular lens power calculation according to the anterior chamber depth in short eyes. Am J Ophthalmol. 2014;157(4):818-824.e2.