

In China, where I practice, the China Food and Drug Administration (CFDA) approved the Visian ICL V4c and the Visian ICL V4c Toric (now EVO Visian ICL and EVO Visian ICL Toric; STAAR Surgical) in October 2014. From my point of view, the approval was supposed to be fairly easy, as the addition of the KS-Aquaport—a hole in the center of the lens that is designed to restore more natural aqueous flow to the eye—made the need for peripheral iridotomy/iridectomy in conjunction with the surgery obsolete. And, in my personal experience, the lens continued to provide my patients with the same excellent visual outcomes postoperatively.
Just one short month after the CFDA approved these lenses, I was fortunate enough to implant the first toric lens of this kind in a 27-year-old man who worked as a teacher. Even from that early experience, I was extremely impressed with the visual quality that the EVO Visian ICL can provide. This specific patient had a refraction of -7.50 -2.00 X 165º OD and -10.50 -2.25 X 165º OS preoperatively, with central corneal thicknesses of 501 μm OD and 506 μm OS. His visual acuity was 0.9 logMAR OU. After surgery, the patient’s visual acuity improved to 1.2 logMAR OU, and he had no pain and no complaints of glare or halos.
In the following years, I continued to see consistently excellent results with the lens that is now known as the EVO Visian ICL. In addition to a low incidence of glare and halos postoperatively, it seemed as if patients did not complain of visually disturbing higher-order aberrations (HOAs) and were able to achieve highly stable optical and retinal image quality.
VISUAL QUALITY ASSESSMENTS
In attempt to better assess these three components of visual quality (HOAs, intraocular scattering and optical quality, and glare and halos) after EVO Visian ICL implantation, I decided to conduct a study of my past patients.
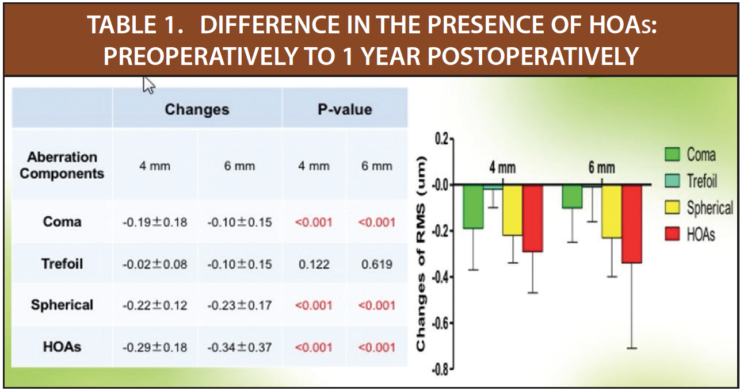
HOAs. The mean age of patients (n=17) included in my evaluation of HOAs after EVO Visian ICL implantation was 26.76 ±5.15 years (range, 20–37 years). Preoperatively, the mean spherical equivalent (SE) in this group of 34 eyes was -12.24 ±3.30 D (range, -5.50 to -18.00 D). Coma, trefoil, spherical aberrations, and total HOAs in each patient were measured preoperatively and at 1, 3, 6, and 12 months postoperatively. In short, all four measurements significantly decreased after implantation of the EVO Visian ICL, both at 4- and 6-mm pupil sizes (Figure 1). And, from 1 month to 1 year postoperatively, all measurements were relatively stable, again both at 4- and 6-mm pupil sizes (Table 1).
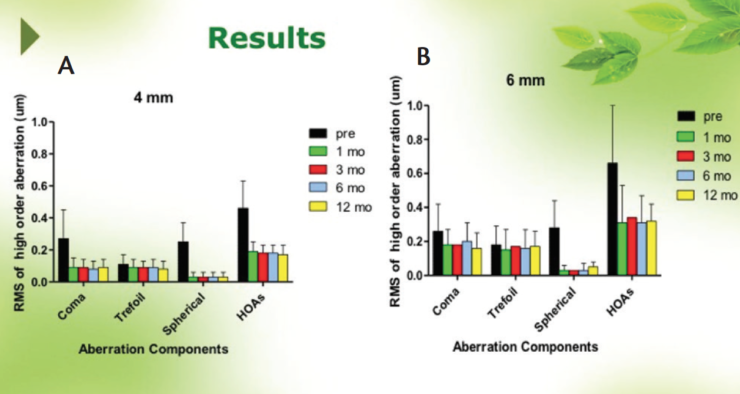
Figure 1. Coma, trefoil, spherical order aberrations, and HOAs at 4-mm (A) and 6-mm (B) pupil sizes.
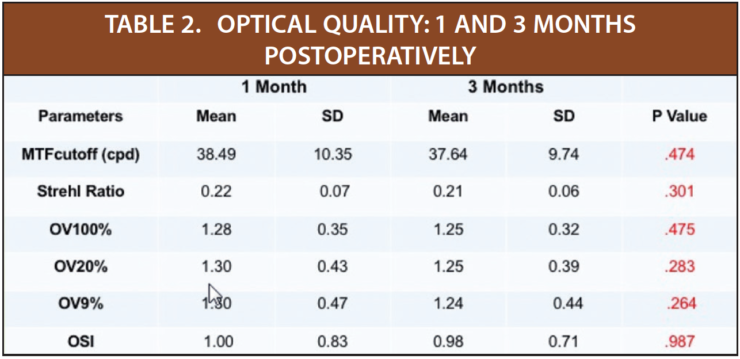
Intraocular scattering and optical quality. In the group of 35 patients with moderate to high myopia included in my evaluation of intraocular scattering and optical quality, the mean age was 28.13 ±6.05 (range, 18–40 years*) and the mean preoperative SE was -12.24 ±3.31 D (range, -5.50 to -20.50 D). Refractive outcomes and optical quality was measured in 35 eyes at 1 and 3 months postoperatively with the OQAS II (Visiometrics), a double-pass optical quality analysis system. As seen in Table 2, patients achieved excellent optical quality by 1 month postoperatively, and that optical quality was stable through 3 months postoperatively. We also found better retinal image quality and lower intraocular scattering in the eyes with lower myopic errors.
Glare and halos. I evaluated the presence of glare and halos in 56 eyes of 28 patients with a mean age of 25.46 ± 6.48 years (range, 18–45 years). The preoperative SE in this group was -10.28 ±2.79 D (range, -3.25 to -18.00 D). The MonCv3 Vision Monitor (Metrovision), a multifunctional perimeter, was used to detect glare and halos preoperatively and at 1 week and 1 month postoperatively. Looking into the MonCv3, patients watched three radial lines, each containing 10 letters, emerge from the periphery toward the glare surface. Also visible were 10 rings at intervals of 33 minutes of arc and a distance of 2.5 m. Using three different luminance levels (1, 5, and 100 cd/m2) to represent night, dusk, and daytime, respectively, optotypes were presented on the screen at a distance of 2.5 m.
All patients reported considerable glare at the initial preoperative assessment, specifically because of the thick spectacle lenses required for the correction of moderate to high myopia. Although glare continued to be obvious to patients at 1 week postoperatively in both night and dusk luminance levels, it was alleviated by 1 month postoperatively. This result indicates that patients can adapt to glare, without any additional treatments, shortly after implantation of the EVO Visian ICL.
Regarding halos, whereas preoperatively the halo size negatively correlated to the SE, postoperatively, it negatively correlated to the power of the EVO Visian ICL and correlated to the scotopic pupil size (Figure 2).
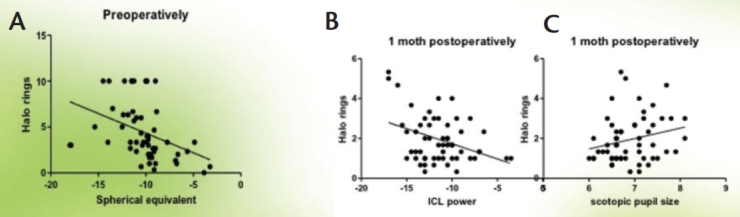
Figure 2. Preoperatively, halo size negatively correlated to SE (A); postoperatively, it correlated negatively to ICL power (B) and correlated to scotopic pupil size (C).
STUDY CONCLUSIONS
From the studies of HOAs, intraocular scattering and optical quality, and glare and halos after EVO Visian ICL implantation, I have concluded that implantation of this phakic lens is safe and effective and that visual quality is stable postoperatively in patients with moderate to high myopia. Furthermore, my patients have all been able to attain excellent and stable postoperative optical within 1 month after lens implantation, as well as a decrease in the presence of HOAs.
Although patients with lower myopic errors tended to achieve better retinal image quality and lower intraocular scattering postoperatively than those with higher errors in these studies, I do believe that the EVO Visian ICL is an excellent choice for any patient who presents with moderate to high myopic errors. I have witnessed the incredible outcomes that all of my patients have achieved, regardless of their preoperative refractions, with many exclaiming that the EVO Visian ICL has changed their lives. It is for these reasons that I will continue to enthusiastically recommend the EVO Visian ICL to my patients when indicated.


