


Sponsored by
Oertli Instrumente AG, Switzerland

Several benefits of combined phacoemulsification with IOL placement with vitrectomy procedures have been described in the literature, including decreased visual rehabilitation and increased convenience to the patient because a second procedure is avoided. There may be additional advantages of performing phacovitrectomy in patients with complicated retinal pathology where clear visualization is of great benefit. As well, the risk of developing a cataract after vitrectomy has been well documented, especially when a tamponade has been used.1-3 Some authors have described the development of cataract after vitrectomy as an inevitability,4 thus suggesting a prophylactic role in some cases for removing the lens in conjunction with posterior segment surgery.
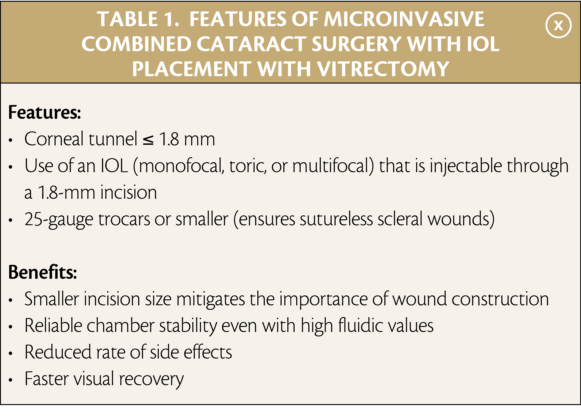
The increasing popularity of phacovitrectomy is incidental with advances in cataract and retinal surgery techniques and technology that have made it possible to perform meticulous and precise surgeries through small openings to reduce the risk of inducing trauma or complications. The Oertli OS4 surgical platform introduces new possibilities for surgeons interested in phacovitrectomy to perform microinvasive combined surgery
(Table 1). The greatest benefit of this functionality with the OS4 is the outstanding chamber stability even when using high fluidic values, resulting in a reduced rate of side effects and faster visual recovery.
EASYPhaco Technology
An advanced cataract removal modality available only on Oertli platforms, easyPhaco describes the way in which several features work together to provide the surgeon the ability to gain great holding strength at the tip via concentrated axial phaco energy, but with minimal turbulence and thorough fragment aspiration, even with dense nuclei. The result is minimal trauma to the eye, faster healing, and less chance of inducing astigmatism. Moreover, the incision remains stable and the cornea clear so that the surgeon can work in the posterior chamber if necessary.
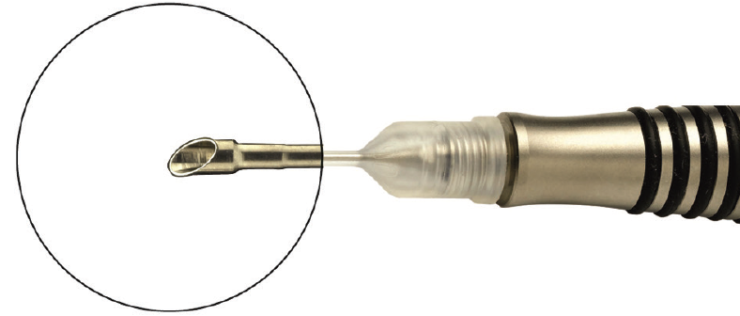
Figure 1. An important component of easyPhaco is the easyTip CO-MICS, which is ideal for sub-2.0 mm surgeries.
An important component of easyPhaco is the easyTip CO-MICS, which is ideal for sub-2.0 mm surgeries (Figure 1). It has been specifically designed for operating through 1.6 to 1.8 mm incisions without compromising efficiency and chamber stability, and it is safe for use with vacuum rates up to 550 mmHg and flow of up to 30 ml. Compared with traditionally designed phaco tips, the easyTip CO-MICS delivers more irrigation flow without increasing the size of the tip through the use of larger internal lumen of the irrigation path that surrounds a slightly smaller aspiration path. Versions of the phaco tip are also available in a 2.2-mm size (for use with 2.2 to 2.4 mm incisions, vacuum up to 650 mmHg, and flow up to 60 ml) and a 2.8-mm size (for use with 2.8 to 3.2 mm incisions and maximum vacuum and flow) (Figure 2).
easyTip Comparison

Figure 2. easyTip CO-MICS, easyTip 2.2 mm, and easyTip 2.8 mm.
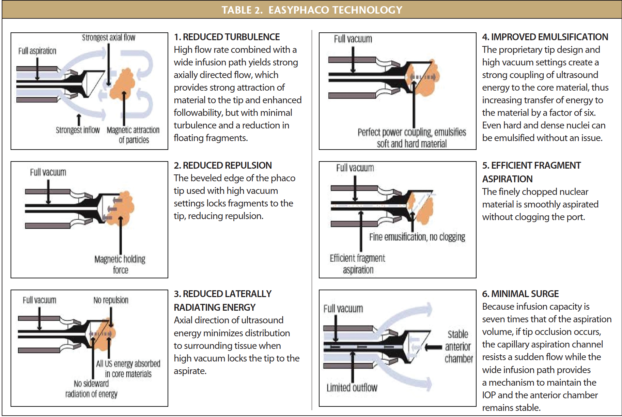
When combined with the advanced High Definition Dynamic Direct Control (HDC) fluidics and other features of the OS4 platform, easyPhaco provides distinct benefits: reductions in turbulence, repulsion, and laterally radiating energy, with corresponding improvements in emulsification and more efficient fragment aspiration, but with minimal surge (Table 2).
Different Pumps for Different Surgical situations
The OS4 is equipped with three different pump modes: peristaltic, Venturi, and SPEEPMode. Surgeons are likely already familiar with peristaltic and Venturi pumps. Many have already staked their preference for one or the other. In truth, each of these pumps may be useful for different purposes, and surgeons may benefit from the ability to quickly switch between them. In addition, the OS4 provides surgeon the ability to use a third modality called SPEEPMode (Speed + Precision).
The SPEEPMode is based on a peristaltic pump, in which vacuum rate is relative to flow. However, in SPEEPMode, the flow is adjustable and vacuum is controlled with the pedal. Additionally, the machine reduces flow rate before maximum vacuum is achieved, thereby creating a strong—but also gentle and precise—aspiration.
The advanced HDC fluidics on the OS4 includes an active infusion feature, which I use in almost every surgery, even in phacoemulsification because it delivers additional safety. During retinal surgery, active infusion helps prevent sudden collapse of the chamber during vitrectomy or when the globe is depressed.
A Versatile System
The sum total of the features of the OS4 and the equipment used with it is a comprehensive and versatile system that is useful for any kind of surgery. Its best features make it possible to safely and effectively perform microinvasive combined cataract surgery with IOL placement and vitrectomy. The availability of three different pump systems and the fact that the surgeon can change the pump system based on preference, and even during the same surgery, adds an unparalleled degree of flexibility.
Every surgeon has his or her own preferences and settings, but the value of having such a versatile platform is that one does not need to relearn surgery to use the OS4. Instead, the platform can be adjusted to the needs of the surgeon. When I am performing combined microinvasive surgery, I perform the phaco step with the Venturi pump, aspiration of the cortex with SPEEPMode (especially if there are weak zonules), the core vitrectomy with Venturi, and then I switch to SPEEPMode for work in the peripheral vitrectomy.
Conclusion
The bottom line is that combined procedures with the OS4 results in tight incisions that heal completely, regardless of the incision size—and there is tremendous benefit for postoperative recovery when sub-2.0 mm incisions are employed. For the vitrectomy portion of the procedure, Oertli’s sharp trocars (Figure 3) help maintain the integrity of the incision, preventing leakage both during and after surgery.

Figure 3. Caliburn 25G cannula system, one step, self-sealing.
1. Hsuan JD, Brown NA, Bron AJ, et al. Posterior subcapsular and nuclear cataract after vitrectomy. J Cataract Refract Surg. 2001;27:443-444.
2. Thompson JT. The role of patient age and intraocular gases in cataract progression following vitrectomy for macular holes and epiretinal membranes. Am J Ophthalmol. 2004;137:250-257.
3. Federman JL, Schubert HD. Complications associated with the use of silicone oil in 150 eyes after retina-vitreous surgery. Ophthalmology. 1988;95:870-876.
4. Villegas VM, Gold AS, Latiff A, et al. Phacovitrectomy. Dev Ophthalmol. 2014;54:102-107.