

I have probably been working with astigmatism correction at the time of cataract surgery longer than any other surgeon in the world. In the early 1980s, when most were concerned with surgically induced astigmatism, I was researching ways to reduce preexisting astigmatism. I eventually performed the first astigmatic keratotomy at the time of cataract surgery, which I think was the first true refractive cataract surgery procedure, and reported the promising results of my series at the Welsh Cataract Congress in Houston in 1984.
Astigmatic keratotomy was certainly an effective method for reducing preexisting astigmatism during cataract surgery; however, it lacked accuracy because we could not guarantee precise incision depth nor control healing. When the toric IOL was introduced, I was hopeful that the Art of incisional surgery would be transformed into a precise Science. But this was not the case.
Once Douglas D. Koch, MD, discovered the contribution made by posterior corneal astigmatism, I believed that the missing link had been found. Still, the penetration for toric IOLs remained dismally low at about 7% to 8% in the United States and about 10% globally (data on file with Alcon). One deterrent to toric IOLs had been the inaccuracy of preoperative marking, identifying the target meridian, and then aligning the lens in surgery.
AN IDEA IS BORN
After implanting a series of toric lenses, I reached several conclusions. First, marking the major meridia before surgery and the target meridia with ink in the operating room was problematic. Not only could the marks be off axis by 10º or 15º, but the ink could diffuse or completely disappear. Second, I became aware that every patient has unique iris landmarks such as crypts, nevi, pigment, holes, Brushfield spots, stromal patterns, and ridges.
Three Helpful Hings for Iris Fingerprinting
Hint No. 1
A high-resolution photograph of the iris should be taken at the slit lamp, during the patient’s original examination. The patient’s pupil must be dilated so that the landmarks appear similar in surgery, the patient’s head must be oriented properly, and the patient must be looking far away and straight ahead.
With this technique, the eye will be oriented properly when the image is captured. The Lenstar (Haag-Streit) and the IOLMaster 700 (Carl Zeiss Meditec) provide this information as an integral part of the biometry measurement accurately and efficiently.
Hint No. 2
Bring a printed image into the operating room, either on paper or on a computer.
Hint No. 3
Never depend on one technology alone to orient a toric IOL—regardless of the technology you use, whether it is iris fingerprinting, Callisto Eye (Carl Zeiss Meditec), or Verion (Alcon). With iris fingerprinting, I still ask my nurses to make an ink mark at the 6-o’clock position in the preoperative area; with a more sophisticated technology, like Verion or Callisto Eye, I always have iris fingerprinting in case something happens to interfere with registration.
Initially I tried using limbal vessels as landmarks, but these would often blanch when the neosynephrine was instilled to dilate the pupil. Then I started to record the major landmarks on the iris by taking a photograph at the time of the initial examination, when the pupil was dilated. Micron Imaging developed the original software that would allow me to touch a cursor over a landmark and the degree at which it was located would be printed on the photograph. Additionally, a target line could be added to represent the exact alignment for the toric IOL. This photograph was taken to the operating room and placed on the microscope, so I always had confidence in my orientation and lens alignment.
I later approached the president of Haag-Streit, Dominik Beck, PhD, and he improved upon the initial technology to develop the Osher Toric Alignment System (OTAS). Sophisticated technologies such as Callisto Eye (Carl Zeiss Meditec) and Verion (Alcon) using similar principles to my original idea for landmark identification were introduced. Other less expensive options of iris fingerprinting were developed by Eye Photo Systems. A similar system with registered information of the planned axis of implantation, incision location, and size as well as measurement data on high-resolution images of the patient’s eye is available on the Lenstar biometer (Haag-Streit).
ADVANTAGES
The advantages of iris fingerprinting include cost, simplicity, and efficiency of time. Compared to more expensive technologies, I have found that fingerprinting is extremely accurate for several reasons. With fingerprinting, it is unneccesary to guesstimate the major meridia and mark with ink. (However I still ask the nursing staff to place an ink mark at the 6-o’clock position as a “belt-and-suspenders” approach.) I have considerable experience with limbal registration, having introduced Verion and more recently becoming a fan of Callisto. One drawback of these technologies, however, is that they depend upon accurate vessel registration. This can be lost if the limbal anatomy becomes altered by conjunctival ballooning from balanced saline solution during phacoemulsification or irrigation/aspiration, chemosis from a subconjunctival anesthetic, or a subconjunctival hemorrhage. We have published a technique for restoring the limbal anatomy should one of these complications occur.1
Alternatively, once you are oriented using iris landmarks, fingerprinting is foolproof. Nothing changes during surgery because the dilated pupil is the same in the operating room as it was during the initial examination. For tips in the use of iris fingerprinting, see Three Helpful Hints for Iris Fingerprinting.
CONCLUSION
Regardless of which technology is preferred, I strongly recommend a “safety net,” as having at least two options available can help to ensure precise toric IOL placement in every circumstance. In my case, I use ThermoDot, which I developed with Beaver-Visitec, to place two tiny cautery marks on the target meridian at the limbus. The ink marks do not diffuse or disappear like ink. I also have an ink mark at the 6-o’clock position, a fingerprinting photograph hanging from my microscope (Figure 1), and the luxury of Callisto and Holos Intraop (Clarity Medical). While this is overkill, I believe that many more surgeons would use toric IOLs if they had the confidence that they were achieving accurate alignment in every case.
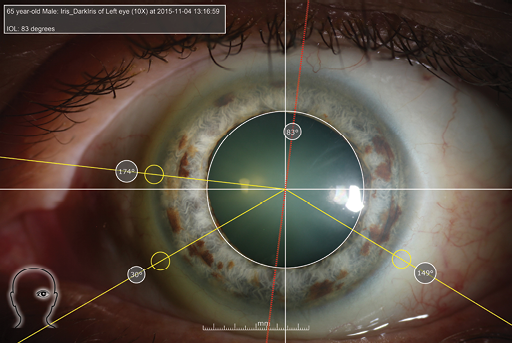
Figure 1. Iris fingerprinting: The white lines indicate the major meridia, the yellow lines show the locations and degrees of the edges of iris nevi, and the red line shows the target meridian at which the toric IOL will be aligned.
For more than a decade, I have been predicting that toric IOLs would become the standard of care. I am confident that, eventually, every refractive cataract surgeon will feel comfortable with this lens technology.
1. Avakian A, Osher RH. Rescue technique for salvaging toric intraocular lens alignment. J Cataract Refract Surg. 2012;38(10):1716-1781.


