
Writing about how to become a good refractive surgeon is indeed a difficult task. I prefer to leave it to my patients and colleagues to judge my capabilities. In this article, however, I will share with you 10 points to consider to help you evaluate your practice and achieve better refractive results and happier patients.
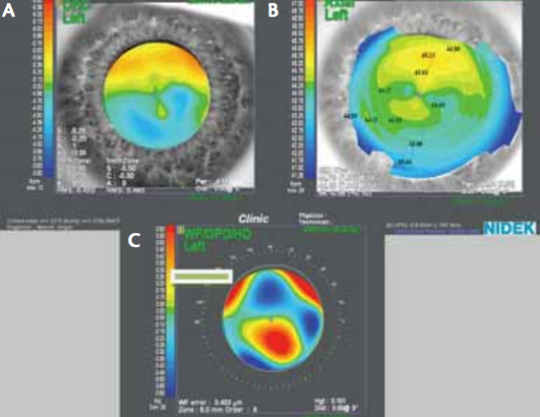
Figure 1. (A) Refractometry shows difference in myopia in upper and lower part of pupil, but no clinical astigmatism. Irregular astigmatism (B) resulting in HOAs and (C) coma.
NO. 1: UNDERSTAND THE OPTICS OF THE EYE
Before caring for any refractive patient, it is crucial to have a good understanding of the optics of the eye. When discussing optics with beginning refractive surgeons, it is interesting to notice the difficulty they have differentiating with-the-rule, against-the-rule, irregular bowtie, and skew-deviation astigmatism. Knowing the influence that higherorder aberrations (HOAs), such as spherical aberrations and coma, have on surgical outcomes and on quality of vision will aid in your analysis of pre- and postoperative visual complaints (Figure 1). All of these factors affect the functional behavior of our patients and their quality of vision.

Figure 2. Diagnostic roundabout for patients.
NO. 2: DIAGNOSTIC INSTRUMENTS
Proper diagnostic instruments for preoperative evaluation assist us in investigating the optics of the eye and excluding eye diseases that could influence our results (Figure 2). My preoperative examination includes automatic keratorefraction, topography, aberrometry, pupillometry, endothelial cell count, Scheimpflug tomography (including corneal thickness map and anterior and posterior elevation maps), optical biometry, subjective blurred refraction, near vision assessment, Amsler grid, Schirmer test, and cyloplegic refraction as well as dilated fundus examination. If any retinal disease is suspected, optical coherence tomography of the macula is performed. Proper preoperative examination will aid in your decision making and help eliminate possible postoperative surprises.

Figure 3. Latest-generation refractive femtosecond and excimer lasers (Refractive Suite from Alcon Laboratories, Inc.).
NO. 3: SURGICAL INSTRUMENTS
Once a treatment is scheduled, be sure to work with the latest-generation tools, including femtosecond lasers or microkeratomes, excimer lasers (Figure 3), phaco machines, properly functioning microscopes, and intraocular devices such as IOLs and capsular tension rings. Refractive surgery involves treating patients whose corrected visual acuity is 20/20, and every effort should be made to maintain or improve that level of vision postoperatively. Be part of a well-educated team of nurses and technicians; this will improve your results, make your patients feel safe, and alleviate stress in your practice and life.
NO. 4: CHAIR TIME
A great deal has been written about chair time. Preoperative chair time is a major issue in establishing a good doctor-patient relationship. In our practice, patients receive preoperative information through leaflets and educational videos. After the preoperative examinations have been performed by the technicians, the doctor converses with the patient, and together they decide on the best treatment plan for the patient’s situation. In fact, every patient receives a personalized approach, not always by correcting his or her HOAs, but by choosing the right treatment for a specific refractive problem.
In patients with presbyopia, there are multiple therapeutic choices, including corneal inlays, laser vision correction (eg, presby-LASIK, monovision), and accommodating and multifocal IOLs. For these patients, a thorough discussion is warranted. During this conversation, the doctor should listen to the patient, identify his or her needs, propose the best solutions, and provide evidence for this choice. It is not always up to the patient to decide which treatment is best, as he or she is not well versed in refractive surgery (or, at least, our knowledge and experience should be greater). After all, patients often feel greater comfort and reassurance when the doctor is in charge of the situation. We have learned that patients are not always happy about leaving our practices with a variety of possible options, as this only raises more questions for them.
NO. 5: CHOICE OF SURGICAL POSSIBILITIES
It is essential that every refractive surgeon be able to offer a wide variety of surgical options, whether performed by him- or herself or by an experienced colleague. Using an excimer laser to treat a 60-year-old 4.00 D hyperopic patient with LASIK without discussing the possibility of refractive lens exchange (RLE) with or without a presbyopia-correcting IOL is not up to date. On the other hand, doctors performing RLE without access to an excimer laser could leave patients disappointed after having reached near emmetropia.
Does this mean that we should offer every possible treatment available on the market? Our practice tries to offer the best possible treatment options for surgery with evidence of safety and efficacy in peer-reviewed journals. Interesting new therapies—corneal inlays, intrastromal femtosecond laser procedures, for instance—with short follow-up are monitored closely but are not immediately implemented into our practice. This defensive approach is in the best interests of our patients. We will not be the first center to try a new treatment in demanding patients with 20/20 vision; however, we will not be the last to offer an established treatment strategy, either.
NO. 6: TREATING PATIENTS LIKE FAMILY
Every patient should be treated as if he or she were a close relative. The surgeon should be convinced of the safety, outcome, and realistic goals to be achieved when offering treatment options. Take into consideration the patient’s age, occupational needs, leisure activities, and hobbies. Also review the patient’s general medical history to exclude possible adverse effects of surgery, and check for possible ocular comorbidities that could influence your outcome.
NO. 7: COMMUNICATION WITH COLLEAGUES
Stay tuned in to the outcomes achieved with different therapies and treatment options by attending congresses, speaking with colleagues in your subspecialty, and reading the literature. Increased knowledge is a good filter for deciding among effective therapies and interesting new technologies. Professional forums on the Internet (eg, the forum of the International Society of Refractive Surgery) may help us to treat troublesome cases and reassure us about what we propose to our patients.
NO. 8: TREATMENT OF COMPLICATIONS
Modern refractive surgery is considered to be safe. However, although rare, complications are inevitable in any kind of surgery. Be prepared for the worst-case scenario and know how to manage it properly. The difference in capability among refractive surgeons is often how complications are handled. To ensure that you are prepared to handle any complication, a well-equipped operating room stocked with a range of tools and devices to aid in unforeseen events should be available. Train your staff to cope with such situations. Our staff attends national and international meetings on a regular basis to learn about possible complications and new approaches.
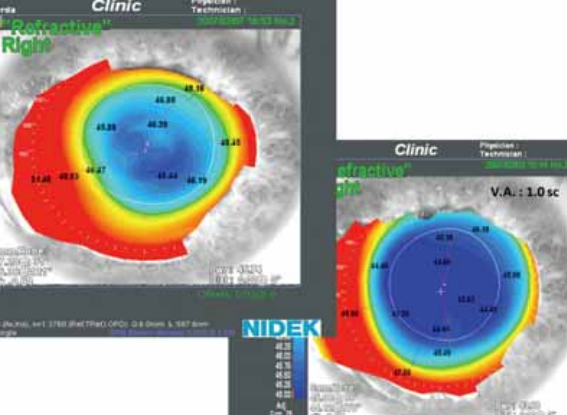
Figure 4. Increasing optical zone with topography-guided LASIK for
improvement of night vision problems.
NO. 9: POSTOPERATIVE CARE
Refractive surgery does not end once the procedure is completed. Follow your patients postoperatively. Reassure them about the results, and help them handle possible adverse effects. Let them know you are there for them and will use all of your knowledge and skills to help them achieve the intended result. Often, over time, this reassurance can turn the unhappy patient into a happy patient without requiring further treatment. If necessary, propose a surgical plan to enhance the patient’s result (Figure 4), explaining the risk-to-benefit ratio, or refer the patient to a trustworthy colleague who has more expertise in handling a certain adverse effect.
NO. 10: ECONOMICS OF REFRACTIVE SURGERY
The costs of installing proper diagnostics and therapeutics are high. Simultaneously building a Class I operating room and establishing a well-trained staff exceeds even several times these expenses. Therefore, economics is an integral part of any refractive surgical practice. Never start your own refractive center without a good financial plan. Be sure your numbers allow you to afford a refractive practice offering all possible treatment options.
Economics should never drive you or your patients toward a certain refractive procedure; only the knowledge of having offered the best possible treatment will satisfy you both. This same happy patient will spread the word and help the growth of your practice.
If, economically, your aims are too difficult to achieve on your own, try joining a larger ambulatory refractive surgery center. This will give you access to diagnostic and therapeutic technologies, keeping your standards high and giving you a better chance to make your patients happy. Otherwise, you may be pushed into overtreatments due to financial obligations, or you may be forced to skimp on quality to survive financially. Overall, this scenario will ruin your goals and will leave you a frustrated surgeon.
CONCLUSION
These 10 points are well known to any experienced refractive surgeon, but they are crucial in evaluating your practice. Giving the best of your abilities and knowledge and working to make your practice a premium clinic that offers high-standard medicine in a relaxed and pleasing atmosphere should be an achievable goal. These tips may serve you not only in being a good refractive surgeon, but also in striving to become a better refractive surgeon every day.
TAKE-HOME MESSAGE
- Listen to and reassure your patients of your dedication to their care, which should continue postoperatively.
- Strive to practice in a setting that offers access to a range of diagnostic and therapeutic instruments and treatments.
Guy Sallet, MD, FEBOphth, practices at Ooginstituut in Aalst, Belgium. Dr. Sallet reports that he is a consultant to Alcon Laboratories, Inc. He may be reached at tel +32 53 21 68 39; e-mail: dr.sallet@ooginstituut.be.