
Nuisance during physical activities, hindrance of wearing glasses, contact lens irritation—these are among the many issues that prompt an increasing number of people to seek freedom from their glasses or contact lenses. For patients interested in laser vision correction, several treatment options are available to reduce dependence on glasses or contact lenses and thus improve quality of life. The latest of these is ReLEx SMILE (Carl Zeiss Meditec), which requires no flap, is associated with no pain and quick recovery, and is fully computer-operated using the femtosecond laser. The procedure was introduced in Europe and Asia in 2012 as an alternative to LASIK for the treatment of myopia or myopic astigmatism. In the United States, clinical trials for FDA approval of SMILE are under way.
As of 2014, more than 125,000 SMILE surgeries have been performed by about 400 users in more than 40 countries. With almost 3 years of experience with SMILE at our center, we have done more than 400 cases but have yet to perform a retreatment; however, the need for enhancements can occur.
THE TECHNIQUE
SMILE, short for small incision lenticule extraction, is a minimally invasive technique performed with the VisuMax femtosecond laser (Carl Zeiss Meditec). With this approach, the disadvantages of older laser vision correction treatments are eliminated, yet the advantages remain. The primary advantage is that it is a flapless procedure. Thus, there is reduced risk of dry eye, better long-term stability of the cornea, and no chance of the flap moving or folding. Because SMILE is performed in a closed environment, the procedure is not affected by external factors such as temperature, humidity, and draft. This increases its accuracy.
Surgical approach. At 5 minutes and 1 minute before treatment, patients receive a drop of oxybuprocaine tetrachloride 0.8% in each eye. Povidone-iodine 10% is used to disinfect the periocular skin, and povidone-iodine 5% is used to disinfect the conjunctival fornices at least 3 minutes before the laser treatment. After ensuring the horizontal position of the patient, he or she is transferred under the laser, and the eye is centered under the curved contact lens.
Once the central fixation of the eye is checked, suction is applied. The posterior cut, which is the refractive cut, is performed first, followed by the anterior nonrefractive cut. At the end of the laser procedure, a sidecut incision of 3.3 mm at 135° is created for the lenticule extraction (see Selection of Basic Cutting Geometry). In our experience, the lenticule minimum thickness was 15 µm in all cases, and the optical zone varied between 6.5 and 6.8 mm. The cap diameter was always 0.8 to 1 mm larger than the lenticule diameter, so it varied from 7.5 to 7.8 mm. Intended cap thickness was 120 µm to 140 µm. In all cases, a small contact lens was used.
After the laser procedure, a blunt spatula (Pfäffl Femto FlapLifter; Geuder) is used to open the sidecut and break the remaining tissue bridges. After a small entry is created to the posterior side of the lenticule, the anterior face of the lenticule is freed from the cap. Next, the posterior part of the lenticule is freed. Once the lenticule is completely free, it is extracted from the pocket using Kelman-McPherson Fragment Forceps (Geuder). At the end of treatment, the lenticule is inspected, and the stromal pocket is rinsed using saline. A drop of tobramycin-dexamethasone (Tobradex; Alcon) is applied on the cornea.
Follow-up examinations are at 1 day, 3 weeks, 3 months, and 1 year. The postoperative regimen consists of tobramycin-dexamethasone drops six times per day and artificial tears (Hylo Gel; Candor Vision) six times per day for 2 weeks. Afterward, the use of lubricating drops is allowed if desired by the patient.
Results. All data were used for statistical analysis with the Datagraph medical software program. Three-month results from 122 eyes of 66 patients (mean age, 34 years [range, 18–65 years]; 41.8% male) were reviewed (Figures 1 through 4). Mean preoperative manifest sphere was -5.08 ±1.61 D (range, -10.00 to -2.25 D), and mean preoperative manifest cylinder was -0.74 ±0.73 D (range, -4.25 to 0.00 D). Mean preoperative spherical equivalent was -5.45 ±1.65 D (range, -10.75 to -2.75 D). Three months after SMILE, 100% of eyes had distance UCVA of 20/40 or better, 92% had 20/25 or better, and 78% had 20/20 or better; 97% of eyes were within ±1.00 D of intended correction, and 84% of eyes were within ±0.50 D. Clinical and corneal tomography results were examined at 6 months.
AT A GLANCE
• The primary advantage of ReLEx SMILE is that the treatment is flapless.
• The retreatment rate after SMILE is low, as the
procedure is performed in a closed environment
and is not affected by environmental factors.
• One of the most important requirements for retreatment is that the surgeon avoid the original SMILE interface.
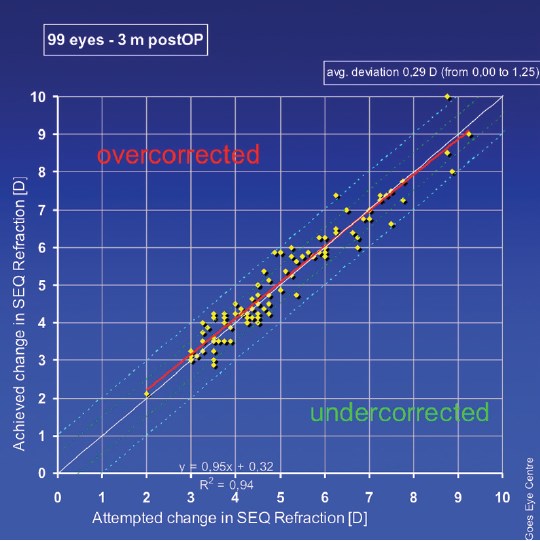
Figure 1. At 3 months, the mean deviation in spherical equivalent was 0.29 D, with almost no differences between medium and higher myopic patients.
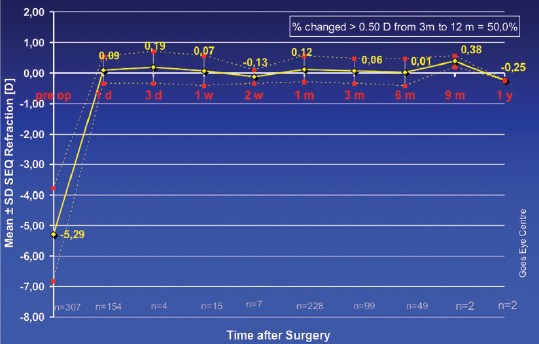
Figure 2. Once stability in spherical equivalent was reached, changes in spherical equivalent were minimal during the first year.
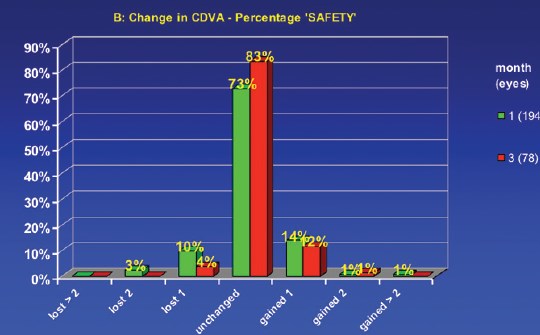
Figure 3. There was no loss of BCVA of more than 1 line at 3 months, and 96% of eyes were stable or gained lines of BCVA.
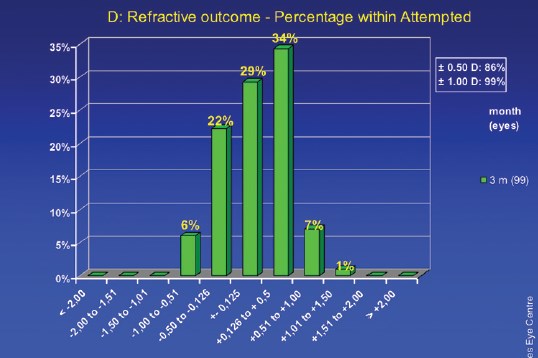
Figure 4. At 3 months, 86% of eyes had a refractive outcome of less than 0.50 D of the attempted correction; 99% had an outcome of less than 1.00 D of the attempted correction.
Retreatment rates after microkeratome or femto-LASIK have been reported as approximately 3% to 5%.1 If the same rate applied to SMILE, we should already have performed 12 to 20 retreatments at our center; however, at this moment, we have performed none. The future will tell whether these results will stand. Nevertheless, it is important to consider the available options for retreatment.
SMILE RETREATMENT OPTIONS
If SMILE is to surpass LASIK as the standard corneal laser surgery procedure, retreatments must be possible and easy to perform. With LASIK, retreatments have always been easy. Generally, relifting the flap is effortless and the visual result is immediate, with patients able to return to work the next day.
With SMILE, the scenario is slightly different. The superficial collagen fibers should not be touched with a retreatment; otherwise, the original advantage of the procedure is lost. Thus, one of the most important requirements for retreatment is that the surgeon stay away from the original SMILE interface. Creation of a second lenticule under the first lenticule would be the ideal solution; however, at present, this is impossible because current software cannot accurately locate the original pocket.
SELECTION OF BASIC CUTTING GEOMETRY

A. Only the sidecut of the hinge is generated (selected)
B. Lamellar ring deeper than existing incision and junction cut to upper side
C. Lamellar ring higher than existing incision and junction cut to lower side
D. Lamellar ring with same depth as existing incision and
junction cut in each direction
PRK. We can choose to perform a standard PRK enhancement on the corneal cap, preserving corneal stability. When PRK is done over a previous SMILE treatment, use of mitomycin C is mandatory in order to prevent the formation of haze.2
LASIK. Another option for retreatment is to perform a standard femto-LASIK procedure using a corneal flap that is thinner than the existing corneal cap thickness. If the corneal cap thickness is 120 µm or less, an ultra-thin femtosecond laser flap should be created, with care taken not to create gas bubble breakthrough or a buttonhole.
Circle. A third retreatment option is to use a technique that recently became available: the Circle procedure (Carl Zeiss Meditec), in which a single sidecut with a clearance zone is used. This turns the original SMILE procedure into a femto-LASIK procedure. The cap is turned into a flap, and the retreatment, performed with the excimer laser, is done on the bed of the original SMILE procedure. Several parameters are adjustable with the Circle technique.
After SMILE, patients undoubtedly prefer flap-based procedures such as femto-LASIK and Circle over PRK. However, corneal stability is better preserved by PRK than by flap-based retreatments.
CONCLUSION
SMILE is my refractive procedure of choice for the treatment of myopia and myopic astigmatism. With SMILE, the retreatment rate seems to be equal to or lower than with LASIK. Evidence suggests that retreatment is both possible and accurate.
- Yuen LH, Chan WK, Koh J, Mehta JS, Tan DT; for the SingLasik Research Group. A 10-year prospective audit of LASIK outcomes for myopia in 37,392 eyes at a single institution in Asia. Ophthalmology. 2010;117(6):1236-1244.
- Ivarsen A, Asp S, Hjortdal J. Safety and complications of more than 1500 small-incision lenticule extraction procedures. Ophthalmology. 2014;121(4):822-828.
- Vestergaard AH, Gronbech KT, Grauslund J, Ivarsen AR, Hjortdal JO. Subbasal nerve morphology, corneal sensation, and tear film evaluation after refractive femtosecond laser lenticule extraction. Graefes Arch Clin Exp Ophthalmol. 2013;251(11):2591-2600.
Frank Goes Jr, MD
- Medical Director of Goes Eye Centre in Antwerp, Belgium
- info@goes.be
- Financial disclosure: None