
Small eyes have anatomic features that can complicate cataract surgery. These eyes have short axial lengths, often associated with shallow anterior chambers. Additionally, the corneal diameter may be less than average, and the effective lens position of an IOL can be more difficult to calculate in these eyes. But there is one great upside: these are hyperopic eyes—often highly hyperopic—and patients with small eyes are dependent on glasses for all activities. When successfully performed in small eyes, cataract surgery can provide these patients with the best uncorrected vision they have experienced in their lives.
PREOPERATIVE EVALUATION
Small eyes have short axial lengths, typically less than 22 mm, and accompanying hyperopia of 3.00 D or more. The anterior chamber can be shallow, with measured depths of 2 mm or less and associated narrow angles. In eyes with advanced cataractous changes, the lens can swell and further narrow the angles.
The cornea should be carefully evaluated for endothelial weakness because there is greater chance of phacoemulsification-induced endothelial cell loss due to the closer proximity of the phaco probe than in normal eyes. Small corneal size can also mean that a standard-sized phaco incision may induce more astigmatic change at the time of cataract surgery.
When axial length is measured in a small eye, a minute error can result in more of a refractive shift than in normal or large eyes. For instance, an axial length that is wrong by 1 mm in a normal-sized eye may induce 3.00 D of error, but in a short eye it may induce 4.00 or even 5.00 D of error.
Difficulty predicting the final effective lens position of the IOL also means that lens calculations are more like estimates. Certain formulas have been shown to be more accurate than others in short eyes. Of the formulas that use two variables, the Hoffer Q tends to perform best for axial lengths less than 22 mm. However, it is advisable to use newer formulas such as the Holladay 2, which incorporates data such as white-to-white size, refraction, and anterior chamber depth, in order to produce more accurate results (see Features of and Considerations in Small Eyes).
LENS CHOICES
One-piece acrylic IOLs are appropriate lens choices for small eyes, as are three-piece acrylic and silicone IOLs, because they all have flexible haptics that allow placement within the smaller-than-usual capsular bag. In some situations, eyes with very short axial lengths may need an IOL power that is particularly high, such as 30.00, 35.00 D, or even more. Because different IOL designs come in different ranges, every effort should be made to identify the most appropriate lens. It is better to have a single IOL with the correct power than to piggyback using two IOLs to achieve the same dioptric strength.
AT A GLANCE
- With careful preoperative planning and appropriate intraoperative techniques, cataract surgery can be successfully performed in small eyes.
- When axial length is measured in a small eye, a minute error can result in more of a refractive shift than in normal or large eyes.
- The cornea should be carefully evaluated for endothelial weakness because there is a greater chance of phacoemulsification-induced endothelial cell loss due to the closer proximity of the phaco probe than in normal eyes.
In the rare eyes in which a power greater than 40.00 D is indicated, it may be advisable to do the surgery in two stages: cataract surgery with implantation of the maximum-power IOL available (40.00 D) in the capsular bag, followed by a second surgery with implantation of a piggyback lens in the ciliary sulcus. This can provide more refractive accuracy because the power of the second IOL, placed in the sulcus, can be determined based on the postoperative refraction after the primary cataract surgery.
Features and Considerations in Small Eyes
Features
•Short axial length, typically less than 22 mm
•Accompanying hyperopia of 3.00 D or more
•Shallow anterior chamber, with measured depths of 2 mm or less
•Associated narrow angle
•Corneal diameter may be less than average
Considerations
• Greater chance of phacoemulsification-induced endothelial cell loss
•A standard-sized phaco incision may induce more astigmatic change at the time of cataract surgery
•Effective lens position of an IOL can be more difficult to calculate
•Small errors in axial length can result in more of a refractive shift than in normal or large eyes
•Choroidal hemorrhage is more common
•Because small eyes typically have shallow anterior chambers, completing the capsulorrhexis and atraumatically removing the nucleus can be challenging
SURGICAL TECHNIQUE
Certain risks such as choroidal hemorrhage are more common in smaller eyes than in normal-sized ones. Additionally, the shallow anterior chamber can make it more difficult to complete the capsulorrhexis and atraumatically remove the nucleus. After creation of an initial paracentesis, the anterior chamber can be inflated with a cohesive ophthalmic viscosurgical device (OVD) in order to create space and deepen the anterior chamber.
In some small eyes, particularly those with coexisting pathology, the anterior chamber can be so shallow as to preclude capsulorrhexis creation. A partial pars plana anterior vitrectomy can be done in order to help deepen the anterior chamber. This procedure, however, is not without risk because it involves creation of a sclerotomy to access the vitreous cavity in a crowded eye. Using a small-gauge vitrectomy unit, a little vitreous can be removed at a time. It is important not to remove too much vitreous, as this can result in an anterior chamber that is too deep. Slowly injecting an OVD while performing the anterior vitrectomy allows precise control.
The corneal endothelium should then be protected with a dispersive OVD. Because the volume of the anterior chamber is small, there is a limited amount of working room during phacoemulsification in small eyes. The closer the phaco probe is to the cornea, the greater the potential for endothelial damage. For this reason, phaco techniques performed within the capsular bag are preferred to extracapsular methods.
Once the cataract is removed and the IOL is inserted in the capsular bag, care should be taken to ensure that the incisions are watertight. Because these small eyes often have smaller-than-normal corneas, the standard-sized phaco incisions may encompass a larger area and arc length and may not seal as well as usual.
Case Study: Successful Surgery in a Small Eye
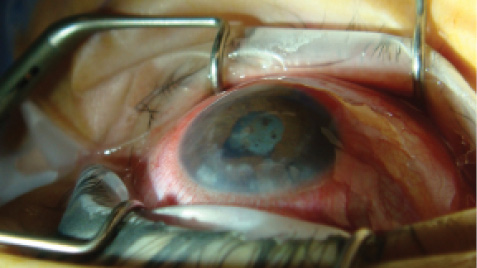
Figure 1. An eye with a less-than-1-mm-deep anterior chamber and a history of angle closure with white cataract formation.
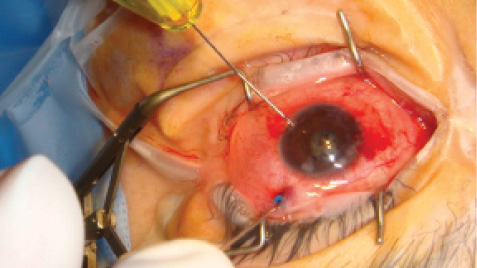
Figure 2. A limited 25-gauge pars plana anterior vitrectomy was performed with the right hand as OVD was injected into the anterior chamber with the left to achieve a normalized depth.
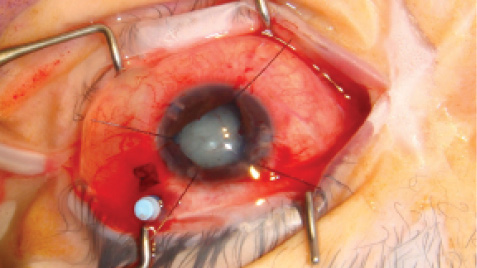
Figure 3. With a deepened anterior chamber, the capsule was stained with trypan blue dye, and a capsulorrhexis was created. Iris hooks were needed to enlarge the pupil for cataract surgery.

Figure 4. At the end of the case, a 40.00 D IOL was well positioned in the capsular bag, the iris hooks were discarded, and the 25-gauge trocar (blue) was about to be removed.
POSTOPERATIVE FOLLOW-UP
Patients with small eyes tend to be particularly happy in the postoperative period because their high degree of hyperopia has been corrected. But there are additional benefits as well, such as restoration of the angle anatomy and lowering of the IOP; these occur because the 4-mm-thick cataract has been replaced by a 1-mm-thin IOL. With careful preoperative planning and appropriate intraoperative techniques, cataract surgery can be successfully performed in these small eyes, as demonstrated in Case Study: Successful Surgery in a Small Eye. n
Uday Devgan, MD
- Private practice, Devgan Eye Surgery, Los Angeles, California
- Chief of Ophthalmology, Olive View UCLA Medical Center, Los Angeles, California
- Clinical Professor of Ophthalmology, Jules Stein Eye Institute, UCLA School of Medicine, Los Angeles, California
- devgan@gmail.com
- Financial disclosure: None