
Development of visually significant cataract after trabeculectomy is typical and expected.1-3 Along with the common pathogenic origins of cataract and glaucoma, other risk factors that have been suggested include age, diabetic status, steroid use, and trauma.4-7 Additionally, glaucoma itself and its treatments—medications, laser, and surgery—have been found to increase the development of cataract. Conversely, cataract development can initiate and/or worsen ocular hypertension and glaucoma.
Performing cataract surgery in an eye with an existing trabeculectomy bleb poses unique challenges. Understanding the bleb morphology and the anatomic setting in which cataract develops requires attention to detail and surgical skills. Cataract surgery can be performed with routine surgical techniques in the presence of a bleb, but special care must be taken to avoid damage to the bleb, especially during placement of the lid speculum and use of a second instrument.
This article details some special considerations for surgical approaches in eyes with cataract and an existing trabeculectomy bleb.
PREOPERATIVE CONSIDERATIONS
Anesthesia. The ideal approach to a patient with an existing bleb would be topical anesthesia with a clear corneal incision (CCI) made away from the bleb. Because these eyes often have advanced glaucoma, retrobulbar block with adrenaline and vigorous massage by external manual compression, superpinky, or Honan balloon must be avoided. If local anesthesia is called for, peribulbar block is the generally preferred modality of anesthesia in these patients.

Figure 1. Careful assessment of bleb site is mandatory.
Assessment. The site of the bleb and extent of the functional bleb should be noted and surgery planned accordingly. Careful preoperative assessment is mandatory for optimal surgical outcome (Figure 1).
Patients should be assessed preoperatively for a number of factors that can predispose them to problems with adequate pupillary dilation. Those with pseudoexfoliation syndrome, posterior synechiae, a history of topical miotic use, and/or a history of systemic a-1 blocker use, with its accompanying increased risk of intraoperative floppy iris syndrome,9 often require iris manipulation to achieve adequate pupil size. Patients with angle closure may have a pupil bound by posterior synechiae due to repeated intermittent angle-closure attacks.
INTRAOPERATIVE CONSIDERATIONS
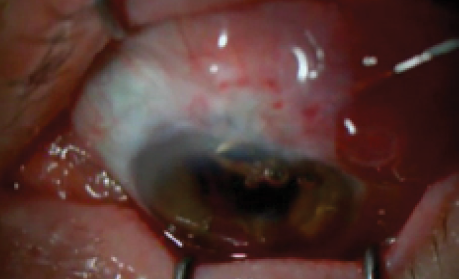
The incision. In the presence of an intact bleb, a temporal CCI represents a safer approach compared with a superior CCI or scleral tunnel. The CCI minimizes conjunctival handling, thereby lowering the risk of bleeding and bleb disruption from incidental damage by a keratome or other surgical instrument (Figure 2). This approach is likely to minimize the chances of bleb scarring and failure.8 In the event of a leaky cataract incision, one can apply a suture without unduly disrupting the existing bleb.
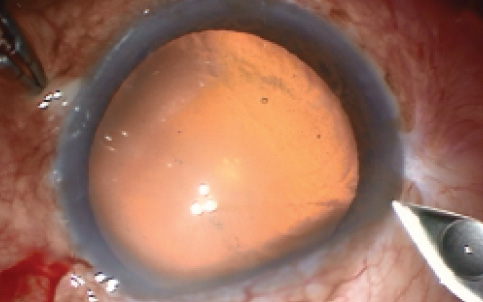
Figure 2. CCI sparing the bleb area.
Pupillary dilation. An inadequately dilated pupil can pose multiple problems during surgery, and manipulation of the iris to achieve adequate pupil size is likely to lead to inflammation—often a detriment to a functioning bleb. Dilation can be achieved by a number of methods, including mechanical pupil stretching with opposing Kuglen hooks, use of a dense ophthalmic viscosurgical device (OVD) such as sodium hyaluronate, iris hooks, and other pupil-expansion devices such as the Beehler Pupil Dilator (Moria) or the Malyugin Ring (MicroSurgical Technology). One should take care when implanting iris hooks and other devices to avoid damage to the existing bleb and to minimize iris manipulation in order to prevent inflammation and fibrin formation, either of which can decrease bleb function.10,11
Anterior vitrectomy. Meticulous care should be taken to assess for zonular disruption and vitreous prolapse in the anterior chamber preoperatively; these can occasionally occur during creation of the peripheral iridectomy in trabeculectomy surgery. Zonular disruption and vitreous in the anterior chamber can cause altered phacodynamics and may lead to infusion-misdirection syndrome intraoperatively and aqueous misdirection postoperatively.12,13 Therefore, if these conditions are present, proper precautions should be taken. A complete anterior vitrectomy should be performed to prevent vitreous prolapse into the sclerostomy and compromised bleb function. Intracameral triamcinolone acetonide can be used to help identify vitreous strands and ensure a complete vitrectomy, which will decrease postoperative inflammation.14
Phacodynamics. Excess filtration from the existing bleb during cataract surgery can alter the phacodynamics and cause frequent shallowing of the anterior chamber. If this occurs, increasing the bottle height and using copious OVD can not only improve phacodynamics but also protect the compromised endothelium, especially in patients with angle-closure glaucoma. Occasionally, filtration into the bleb can lead to conjunctival ballooning and pooling of fluid on the cornea, which may disrupt the surgeon's view. This can be managed by making one or two incisions in the conjunctiva 90° to 180° away from the bleb area.15
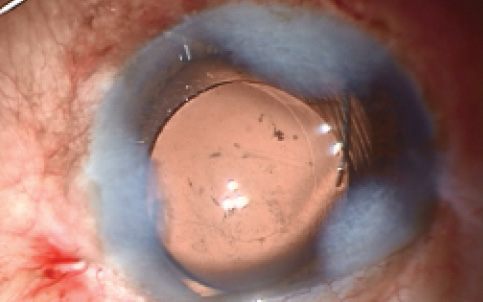
Figure 3. Capsular bag placement of the IOL.
Aspiration. Meticulous care should be taken to aspirate all cortical matter and OVD in order to avoid blockage of the sclerostomy and to minimize postoperative inflammation.16 A Seidel test with fluorescein can be done to avoid overlooking any bleb leakage. If a bleb leak is present, it can be repaired at the completion of cataract surgery.
IOL CHOICE
A variety of IOLs are available, from aspheric monofocal to multifocal and accommodating. However, not all premium IOLs are optimal for use in people with glaucoma. Multifocal lenses can be implanted in patients with mild glaucoma, but those with advanced glaucoma do not benefit from multifocal IOLs because of the resulting reduction in contrast sensitivity and the uncertain influence of these lenses on visual field performance.17,18 An alternative may be an accommodating IOL such as the Crystalens (Bausch + Lomb), which has been observed not to reduce contrast sensitivity, or an aspheric monofocal IOL, which have been shown to improve perifoveal threshold perimetry levels by 4 dB compared with standard IOLs.19,20 Studies have found no difference between blue–light-filtering and nonfiltering IOLs in terms of visual function, including performance on short wavelength automated perimetry (SWAP).21
AT A GLANCE
- Cataract surgery can be performed with routine surgical techniques in the presence of a bleb, but special care must be taken to avoid damage to the bleb.
- After a careful phacoemulsification surgical technique, whatever IOL is chosen, it should ideally be placed in the capsular bag.
- Careful preoperative planning and discussion can establish realistic patient expectations and prepare the surgeon for minor perioperative adjustments and interventions that can promote long-term visual function.
Watch it Now
In the presence of a dysfunctional bleb, slit-lamp bleb revision can be performed at the time of cataract surgery.
Whatever IOL is chosen, it should ideally be placed in the capsular bag (Figure 3). In case sulcus placement of the IOL is necessary, one should avoid placement of a haptic over the peripheral iridectomy, as the haptic may migrate into either the anterior chamber or the sclerostomy and may compromise angle structures.
Generally, angle-supported anterior chamber IOLs should be avoided, as the IOL footplate may disrupt and block the sclerostomy, causing inflammation and, ultimately, bleb failure. In case of inadequate support for a posterior chamber IOL, one may leave the eye aphakic and consider a contact lens trial. If the patient is found to be intolerant to contact lenses, secondary IOL implantation in the form of a suture-fixated, glued, or anterior chamber IOL can be considered.
ADDITIONAL PROCEDURES
If the patient's bleb is dysfunctional, bleb revision (eyetube.net/?v=sugaf) can be performed at the time of cataract surgery. If the bleb is functional, intraoperative application of mitomycin C or 5-fluorouracil may promote bleb function and survival.22,23
Corticosteroids have been found to control inflammation and improve outcomes after cataract surgery in patients with existing trabeculectomy.24 Recently, vascular endothelial growth factor (VEGF)-inhibiting agents, such as bevacizumab (Avastin; Genentech) and ranibizumab (Lucentis; Genentech), have been demonstrated to decrease bleb vascularity and, hence, reduce bleb fibrosis.25
CONCLUSION
The outcomes of cataract extraction with IOL implantation in the presence of a functional trabeculectomy bleb have been evaluated by numerous authors.26-29 In patients with an existing trabeculectomy bleb, cataract surgery can be safely performed; however, patients should be made aware that surgery may hasten bleb failure.27-29 Careful preoperative planning and discussion can establish realistic patient expectations and prepare the surgeon for minor perioperative adjustments and interventions that can promote long-term visual function. n
1. Advanced Glaucoma Intervention Study (AGIS) Investigators. Advanced Glaucoma Intervention Study: 8. Risk of cataract formation after trabeculectomy. Arch Ophthalmol. 2001;119:1771-1779.
2. Molteno ACB, Bosma NJ, Kittelson JM. Otago glaucoma surgery outcome study: long-term results of trabeculectomy—1976 to1995. Ophthalmology. 1999;106:1742-1750.
3. Musch DC, Gillespie BW, Niziol LM, et al; Collaborative Initial Glaucoma Treatment Study Group. Cataract extraction in the collaborative initial glaucoma treatment study: Incidence, risk factors, and the effect of cataract progression and extraction on clinical and quality-of-life outcomes. Arch Ophthalmol. 2006;124(12):1694-1700.
4. Mitchell PG, Cumming RG, Mackey DA. Inhaled corticosteroids, family history, and risk of glaucoma. Ophthalmology. 1999;106:2301-2306.
5. Cumming RG, Mitchell PG, Lim R. Iris color and cataract the Blue Mountains Eye Study. Am J Ophthalmol. 2000;130:237-238.
6. Weih LM, Mukesh BN, McCarty CA, et al. Association of demographic, familial, medical, and ocular factors with intraocular pressure. Arch Ophthalmol. 2001;119:875-880.
7. Leske MC, Wu SY, Nemesure B, Hennis A; Barbados Eye Studies Group. Risk factors for incident nuclear opacities. Ophthalmology. 2002;109:1303-1308.
8. Ernest PH, Tipperman R, Eagle R, et al. Is there a difference in incision healing based on location? J Cataract Refract Surg. 1998;24:482-486.
9. Chang DF, Campbell JR. Intraoperative floppy iris syndrome associated with tamsulosin (Flomax). J Cataract Refract Surg. 2005;31:664-673.
10. Seah SK, Jap A, Prata JA, et al. Cataract surgery after trabeculectomy. Ophthalmic Surg Lasers. 1996;27:587-594.
11. Chen PP,Weaver YK, Budenz DL, et al. Trabeculectomy function after cataract extraction. Ophthalmology. 1998;105:1928-1935.
12. Mackool RJ, Sirota M. Infusion misdirection syndrome. J Cataract Refract Surg. 1993;19:671-672.
13. Ruben ST, Tsai JC, Hitchings RA. Malignant glaucoma and its management. Br J Ophthalmol. 1997;81:163-167.
14. Burk SE, Da Mata AP, Snyder ME, et al. Visualizing vitreous using Kenalog suspension. J Cataract Refract Surg. 2003;29:645-651.
15. Liyanage SE, Angunawela RI, Little BC. Conjunctival sweeping with a squint hook to reduce chemosis. J Cataract Refract Surg. 2007;33:1691-1693.
16. Swan K. Reopening of nonfunctioning filters-simplified surgical techniques. Trans Am Acad Ophthalmol Otolaryngol. 1975;79:342-348.
17. Vingolo EM, Grenga P, Iacobelli L, et al. Visual acuity and contrast sensitivity: AcrySof ReSTOR apodized diffractive versus AcrySof SA60AT monofocal intraocular lenses. J Cataract Refract Surg. 2007;33:1244-1247.
18. Martínez PA, Gómez FP, España AA, et al. Visual function with bilateral implantation of monofocal and multifocal intraocular lenses: a prospective, randomized, controlled clinical trial. J Refract Surg. 2008;24:257-264.
19. Cuthbertson FM, Dhingra S, Benjamin L. Objective and subjective outcomes in comparing three different aspheric intraocular lens implants with their spherical counterparts. Eye (Lond). 2009;23(4):877-883.
20. Tzelikis PF, Akaishi L, Trindade FC, et al. Spherical aberration and contrast sensitivity in eyes implanted with aspheric and spherical intraocular lenses: a comparative study. Am J Ophthalmol. 2008;145:827-833.
21. Kara-Júnior N, Jardim JL, de Oliveira Leme E, et al. Effect of the AcrySof Natural intraocular lens on blue-yellow perimetry. J Cataract Refract Surg. 2006;32:1328-1330.
22. Sharmal TK, Arora S, Corridan PG. Phacoemulsification in patients with previous trabeculectomy: role of 5-fluorouracil. Eye (Lond). 2007;21:780-783.
23. Gutiérrez-Ortiz C, Cabarga C, Teus MA. Prospective evaluation of preoperative factors associated with successful mitomycin C needling of failed filtration blebs. J Glaucoma. 2006;15:98-102.
24. Araujo SV, Spaeth GL, Roth SM, et al. A ten-year follow-up on a prospective, randomized trial of postoperative corticosteroids after trabeculectomy. Ophthalmology. 1995;102:1753-1759.
25. Jonas JB, Spandau UH, Schlichtenbrede F. Intravitreal bevacizumab for filtering surgery. Ophthalmic Res. 2007;39:121-122.
26. Manoj B, Chako D, Khan MY. Effect of extracapsular cataract extraction and phacoemulsification performed after trabeculectomy on intraocular pressure. J Cataract Refract Surg. 2000;26:75-78.
27. Halikiopoulos D, Moster MR, Azuara-Blanco A, et al. The outcome of the functioning filter after subsequent cataract extraction. Ophthalmic Surg Lasers. 2001;32:108-117.
28. Ehrnrooth P, Lehto I, Puska P, et al. Phacoemulsification in trabeculectomized eyes. Acta Ophthalmol Scand. 2005;83:561-566.
29. Derbolav A, Vass C, Menapace R, Schmetterer K, Wedrich A. Long-term effect of phacoemulsification on intraocular pressure after trabeculectomy. J Cataract Refract Surg. 2002;28:425-430.
Pankaj Kataria, MS
- Senior Resident, Advanced Eye Centre, Postgraduate Institute of Medical Education and Research, Chandigarh, India
- pankaj.iyf@gmail.com
- Financial disclosure: None
Sushmita Kaushik, MS
- Additional Professor, Advanced Eye Centre, Postgraduate Institute of Medical Education and Research, Chandigarh, India
- sushmita_kaushik@yahoo.com
- Financial disclosure: None
Surinder S. Pandav, MS
- Professor, Advanced Eye Centre, Postgraduate Institute of Medical Education and Research, Chandigarh, India
- sspandav@yahoo.com
- Financial disclosure: None