
At a Glance
• Application of suture cutback can reduce corneal compression and irregular astigmatism and preserve wound apposition, thereby enabling safe healing and earlier visual recovery.
• In the procedure, the surgeon divides the superficial corneal lamellae along the suture tract, creating a partial thickness corneal groove, and the suture slips into the groove.
Surgeons sometimes face a situation in which a corneal wound has to be secured with sutures until full healing occurs. Common situations include an enlarged phaco incision, PKP, surgeries involving pediatric corneas, wound burn, and corneal laceration. It is often difficult to appose the wound edges sufficiently without causing undue compression of the corneal tissue.
Wound burn and wound dehiscence lead to local flattening, whereas a tight suture leads to local compression and steepening of the cornea.1 The tight suture can induce severe irregular astigmatism and decreased visual acuity. The sutured cornea heals in 6 weeks or more, and once stromal healing has occurred the suture is removed. An intrastromal mattress suture technique that is astigmatically neutral has been described.2 However, most surgeons use radial sutures.
Suture cutback is a simple technique that can reduce corneal compression and irregular astigmatism and preserve wound apposition, thereby enabling safe healing and earlier visual recovery. The procedure can be performed any time after the first postoperative week.
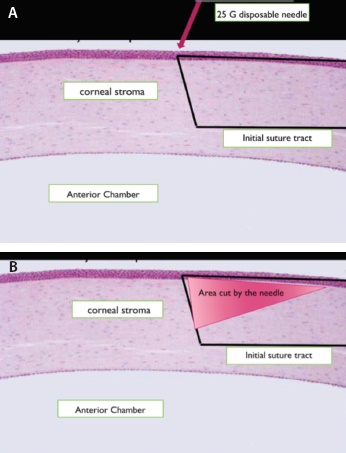
Figure 1. Illustration of the suture cutback procedure: The black line represents the tight suture. The needle enters the stroma at the point where the suture dips into the central cornea. The cut is made from this point toward the sclera along the suture tract (A). The red triangle represents the area cut by the needle (B).
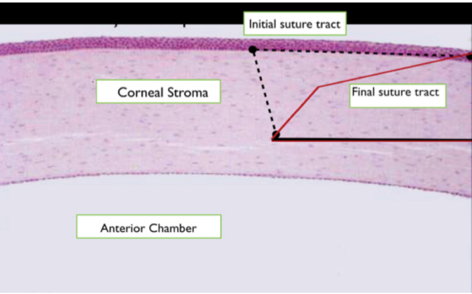
Figure 2. The initially tight suture drops into the groove made by the needle. The suture now takes a shorter path, and there is less compression of the cornea.
In the cutback procedure, the surgeon first divides the superficial corneal lamellae close to and parallel to the suture tract, taking care not to cut the suture. The surgeon creates a partial thickness corneal groove, and the suture slides into this groove. As the amount of tissue compressed by the tight suture is reduced, astigmatism is also reduced. We have used this technique—described herein—successfully in many different surgical situations.
TECHNIQUE
A drop of topical proparacaine HCl is instilled in the eye, twice, 30 seconds apart. The patient is positioned at the slit lamp, and he or she is directed to gaze in the appropriate direction to expose the suture tract clearly. It is best to use oblique illumination with a 1-mm slit beam. A 25-mm long, disposable 26-gauge needle is used to make the corneal groove. The tip of the needle enters the cornea at the point of entry of the suture into the cornea (Figure 1A). A one-third to one-half thickness corneal groove is cut parallel to and close to the suture tract (Figure 1B); care is taken not to cut the suture during the process.
Once the groove is made, the suture will slide into it, and the compression of the corneal tissue is reduced (Figure 2). After each cutback, an immediate change is seen in the central corneal cylinder. The procedure can be repeated to deepen and/or lengthen the groove until sufficient astigmatism is corrected. The cut is never extended into the sclera.
After each cutback, topical lubricant drops are instilled in the eye, and the patient remains seated for a few minutes with his or her eyes closed. Visual acuity and keratometry or corneal topography are repeated until there is evidence that the compression has been relieved. The procedure is painless. The patient continues to use the usual prescribed postoperative eye drops afterward.
SUTURE CUTBACK AFTER RING INSERTION
An 81-year-old man with small pupils, a dense cataract, loose zonules, and significant against-the-rule corneal astigmatism underwent cataract surgery. In order to insert a Cionni Ring (Morcher) to stabilize the capsular bag, the wound was enlarged. The Cionni Ring was anchored with nylon sutures passed through a Hoffman tunnel. A toric IOL was implanted, and the enlarged phaco incision was secured with a single 10-0 nylon suture.
On postoperative day 7, the single tight sclerocorneal suture was seen to be causing severe compression of the cornea, with steepening of the central cornea in the meridian of the suture. Severe irregular astigmatism in the pupillary zone was evident on corneal topography (Figure 1A). The pupil was irregular and enlarged because iris hooks were used during surgery. The patient’s UCVA at this point was 20/200.
Cutback of the tight suture was performed at this visit. After the suture slipped into the groove, topography was repeated. Corneal compression had decreased; however, irregular astigmatism within the pupillary zone was still evident on topography (Figure 1B).
The groove was then made longer and deeper with a second cutback, and the corneal compression was further relieved. On topography, the central steepening had disappeared (Figure 1C). UCVA improved to 20/40 on the same day and to 20/30 a week later.
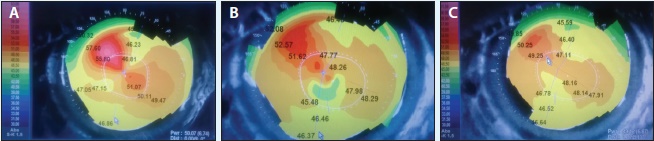
Figure 1. Topography on postoperative day 7, before cutback. The central white line represents the overlay of the pupil on the topography. The pupil is irregular and enlarged because iris hooks were used during surgery (A). Topography after first cutback on postoperative day 7 (B) and after second cutback on postoperative day 7 (C).
CONCLUSION
Our technique of suture cutback is a simple procedure that can be done at the slit lamp. For a case report using the technique, see Suture Cutback After Ring Insertion. Compared with a tight radial suture, which distorts vision, cutting the corneal lamellae along the suture tract permits the suture to slide into the groove in the cornea and relieve corneal compression. The only tools that are needed are a topical anesthetic agent and a 26-gauge disposable needle. Immediate improvement in visual acuity is usually seen. n
1. Gelender H. Management of corneal astigmatism after cataract surgery. Refract Corneal Surg. 1991;7(1):99-102.
2. Alekseev BN, Voronin GV. [Effects of surgical wounds hermetic closure methods in cataract extraction on postoperative corneal astigmatism]. Vestn Oftalmol. 1998:114(1):13-16. [in Russian]
Ramesh Dorairajan, DO, MS
• Ophthalmologist, Sundar Eye Hospital, Chennai, India
• phacochop@hotmail.com
• Financial disclosure: None
Geetha Parasuram, MBBS, DO
• Optometrist, NationWide Vision Center, Arizona
• mail4drgeetha@gmail.com
• Financial disclosure: None
Varshini Ramesh, MBBS
• Resident, Sundar Eye Hospital, Chennai, India
• varshramesh@gmail.com
• Financial disclosure: None