

I had the privilege of being trained in refractive surgery by Dimitri Azar, MD. This giant in ophthalmology was a key figure in refining the original excimer laser surface ablation procedure, PRK. He was the first surgeon to use alcohol to loosen an epithelial flap in such a gentle fashion that he could replace it after photoablation. He was the first to perform this procedure almost 20 years ago, although the term describing it, LASEK, was only later coined and popularized by Massimo Camellin, MD. Moreover, Dr. Azar meticulously examined the influence of alcohol on corneal epithelial cells in cell cultures and animal models to find the most effective and safe concentration of ethanol (18–20%).
In view of this background, my personal perspective on surface ablation may well be biased. However, the literature shows that, even in the early days, surface ablation had excellent and stable clinical outcomes.1-3
SURFACE ABLATION DRAWBACKS
Like many ophthalmologists, I love using new cutting-edge technologies and procedures such as small incision lenticule extraction (SMILE) and femtosecond LASIK, utilizing highly sophisticated eye-trackers and the latest ablation profiles. Surface ablation techniques have two major downsides compared with LASIK and SMILE: These newer procedures provide more comfortable and more rapid visual recovery for most refractive surgery patients.4
At a Glance
• Even in the early days, surface ablation had excellent and stable clinical outcomes.
• Pain management after surface ablation has been improved dramatically with the introduction of innovations including cooling of the eye with ice-chilled salt solution immediately after photoablation, the use of oral triptans, and the use of nonpreserved NSAID eyedrops.
Historically, clinicians have tried to eliminate the disadvantages of surface ablation by introducing variations of the original PRK technique, including (1) LASEK,5,6 using alcohol to create an epithelial flap that is repositioned after photoablation (Figure 1A); (2) advanced surface ablation, using alcohol to remove the epithelium without replacing it (Figure 1B); (3) epi-LASIK, using a microkeratome equipped with a blunt blade to separate the epithelium from the basement membrane; and (4) epithelial Bowman keratectomy (EBK), in which a handheld instrument with a dull tip (Epi Clear; Orca Surgical) is used to remove the epithelium (Figure 1C; www.eyetube.net/?v=eepos). We have evaluated all these modifications of surface ablation and found them to be comparable in terms of pain perception, speed of epithelial closure and visual recovery, haze formation, and final visual outcomes.7-9
Pain management after surface ablation has been improved dramatically with the introduction of innovations including cooling of the eye with ice-chilled balanced salt solution immediately after photoablation (Figure 2); the use of oral triptans, such as sumatriptan, a migraine medication; and the use of nonpreserved NSAID eyedrops.10 Still, patients continue to prefer the wow effects and comforts of LASIK and SMILE.
VARIATIONS OF THE ORIGINAL PRK TECHNIQUE
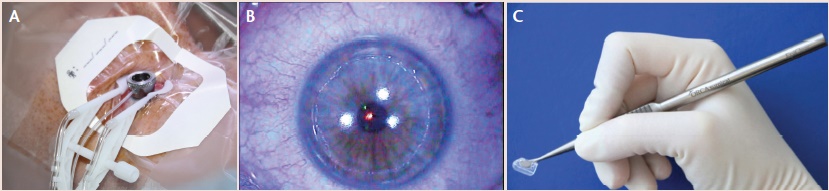
Figure 1. Vidaurri fluid retention ring (Katena) is used for alcohol application in LASEK (A). Circular epithelial defect remains after alcohol-assisted epithelial removal without replacing the epithelium (B). Handheld instrument with a dull tip is used for gentle epithelial removal without chemicals, preserving the Bowman layer (C).
STILL INDISPENSABLE
However, there are good reasons why surface ablations are and will remain indispensable to my daily practice:
Reason No. 1: Surface ablation can provide simultaneous therapeutic treatment together with refractive correction. It can be used in recurrent erosion syndrome or for the removal of subepithelial opacities that either affect vision or make creation of a LASIK flap or SMILE procedure problematic.
Reason No. 2: Surface ablation makes a good retreatment procedure. In recent years, surface ablation on the LASIK flap has become my favorite choice for retreatment, rather than lifting the flap. The reason is that iatrogenic keratectasia has been strongly associated with reablation under the LASIK flap. At times, it may be impossible to determine whether a myopic undercorrection or regression is a stable condition or the beginning of ectasia formation. By ablating on top of the flap, we do not weaken corneal stability any further and avoid this potential pitfall. It is true that surface ablation after LASIK, and especially after SMILE, is more prone to cause haze formation; however, this can be overcome by using mitomycin C 0.02% for 12 to 120 seconds (Figure 3).
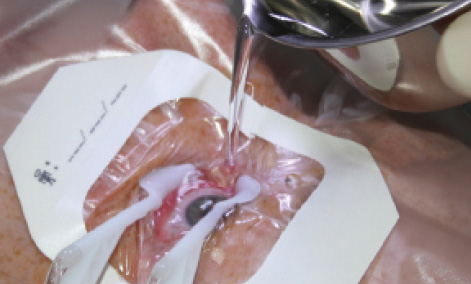
Figure 2. The eye is cooled with an ice-chilled salt solution immediately after photoablation.

Figure 3. Mitomycin C 0.02% is used in a LASEK procedure for 12 to 120 seconds.
Reason No. 3: Surface ablation is gentler to the cornea. In particularly young refractive surgery patients, it may be prudent to be old-fashioned and opt for surface ablation because their corneas may be susceptible to developing keratoconus later, and none of our current diagnostic tools are capable of detecting this genetically fixed precondition. Nevertheless, at present, I would not recommend performing surface ablation in a patient with forme fruste keratoconus in even one eye. On the other hand, there have been anecdotal reports of keratoconic patients with thin corneas who have had PTK or PRK with stable corneal topography for years thereafter. Some speculate that the reason for this observation may be the slight haze formation after uneventful surface ablation, which may represent some sort of strengthening crosslinking of collagen.
Reason No. 4: Surface ablation pairs well with CXL. When performing CXL to treat ectatic eyes, I prefer laser ablation to manual abrasion for epithelial removal. To do this, we first obtain an epithelial thickness map with the Avanti OCT (OptoVue), showing the thinning of the epithelium over the apex and thickening around it. This enables us to smooth the stromal contour by using a limited surface ablation of homogeneous depth to remove the epithelium without sacrificing too much stromal tissue. Kanellopoulos and coworkers have published extensively on a more courageous approach, the Athens protocol, in which anterior corneal topography-guided surface ablations are used to flatten the cone before CXL.11-14
Watch It Now
During the EBK procedure, the Epi Clear device is used to create clear and graduated borders for enhanced healing.
Reason No. 5: Surface ablation can still be performed in the presence of an irregular flap. Surface ablations have saved the day for me multiple times in the past when I created an irregular LASIK flap.15,16 These complications have included short flaps due to suction loss and buttonhole flaps. Instead of waiting several months for the cornea to heal and trying again, in these cases I did not lift the flap but instead performed surface ablation on the irregular flap, after carefully removing the epithelium with alcohol.
CONCLUSION
Clinicians will no doubt continue to refine LASIK and SMILE. No matter how successful these procedures become, however, I am convinced that there will always be good indications that can inherently be better addressed by the first-generation laser treatment: surface ablation. In the long term, with enhanced control of corneal pain perception and improved promotion of epithelial healing, surface ablation may not only survive but thrive. n
1. Taneri S, Azar DT. LASEK: results after 1 year. Retrospective analysis based on the dioptric power matrix for moderate myopic and astigmatic correction [in German]. Ophthalmologe. 2005;102(3):235-240.
2. Taneri S, Feit R, Azar DT. Safety, efficacy and stability indices of LASEK correction in moderate myopia and astigmatism. J Cataract Refract Surg. 2004;30(10):2130-2137.
3. Feit R, Taneri S, Azar DT, Chen CC, Ang RT. LASEK: results. Ophthalmol Clin North Am. 2003;16(1):127-135, viii.
4. Taneri S, Weisberg M, Azar DT. Surface ablation techniques. J Cataract Refract Surg. 2011;37(2):392-408.
5. Taneri S, Zieske JD, Azar DT. Evolution, techniques, clinical outcomes, and pathophysiology of LASEK: review of the literature. Surv Ophthalmol. 2004;49(6):576-602. Review. Erratum in: Surv Ophthalmol. 2005;50(5):502-504.
6. Azar DT, Taneri S, Chen CC. Laser sub-epithelial keratomileusis (LASEK) review and clinicopathological correlations. Middle East J Ophthalmol. 2002;10:54-59.
7. Taneri S, Oehler S. Reply: Epi-LASIK versus LASEK and PRK. J Cataract Refract Surg. 2012;38(4):732-733.
8. Taneri S, Oehler S, Koch J, Azar D. Effect of repositioning or discarding the epithelial flap in laser-assisted subepithelial keratectomy and epithelial laser in situ keratomileusis. J Cataract Refract Surg. 2011;37:1832-1846.
9. Taneri S, Oehler S, Koch J, Azar DT. Epithelium on or off? Cataract & Refractive Surgery Today Europe. October 2010: 27-29.
10. Taneri S. Treating pain after corneal surface ablation. Cataract & Refractive Surgery Today. March 2008: Suppl. 32.
11. Kanellopoulos AJ, Asimellis G. Epithelial remodeling after partial topography-guided normalization and high-fluence short-duration crosslinking (Athens protocol): results up to 1 year. J Cataract Refract Surg. 2014;40(10):1597-1602.
12. Kanellopoulos AJ, Asimellis G. Corneal refractive power and symmetry changes following normalization of ectasias treated with partial topography-guided PTK combined with higher-fluence CXL (the Athens Protocol). J Refract Surg. 2014;30(5):342-346.
13. Kanellopoulos AJ, Asimellis G. Keratoconus management: long-term stability of topography-guided normalization combined with high-fluence CXL stabilization (the Athens Protocol). J Refract Surg. 2014;30(2):88-93.
14. Kanellopoulos AJ, Asimellis G. Comparison of Placido disc and Scheimpflug image-derived topography-guided excimer laser surface normalization combined with higher fluence CXL: the Athens protocol, in progressive keratoconus. Clin Ophthalmol. 2013;7:1385-1396.
15. Taneri S. Epi-LASIK after amputation of a LASIK Flap. J Refract Surg. 2006;22(6):613-616.
16. Taneri S, Koch JM, Melki SA, Azar ST. Mitomycin-C assisted PRK to treat buttonholed LASIK flap associated with epithelial ingrowth. J Cataract Refract Surg. 2005;31(10):2006-2030.
Suphi Taneri, MD
• Director, Center for Refractive Surgery, Eye Department, St. Francis Hospital, Muenster, Germany
• taneri@refraktives-zentrum.de
• Financial disclosure: None