

In cataract surgery, avoiding subluxation or enlargement of an existing subluxation of the crystalline lens is of prime importance. Basic principles in pre- and intraoperative planning can help greatly in decreasing the risk of these events and in managing them if they occur.
It is crucial to be prepared in such cases and to take all precautions to avoid increasing subluxation. These precautions include carefully creating a capsulorrhexis that is appropriately sized and centered, performing gentle intraocular maneuvers, avoiding intracapsular procedures that place stress on the zonules, and taking care to avoid sudden shallowing of the anterior chamber, especially when removing the phaco tip or I/A probe. IOL implantation should be done carefully without exerting stress on the zonules. During surgery, it is important to watch for zonular dialysis so that appropriate corrective action can be taken at the earliest indication.
The capsulorrhexis should be started in the direction of zonular dialysis in order to avoid placing additional stress on the zonules. If this is difficult to accomplish with a cystotome due to anterior capsular laxity, the capsulorrhexis can be continued using microrhexis forceps. The next step is to perform good cortical cleaving hydrodissection, making sure this is done gently to avoid causing stress to the zonules. The surgical strategy to be used is then determined. The extent of subluxation determines the type of surgical intervention. This can be explained with the help of a few case examples, as described throughout this article.
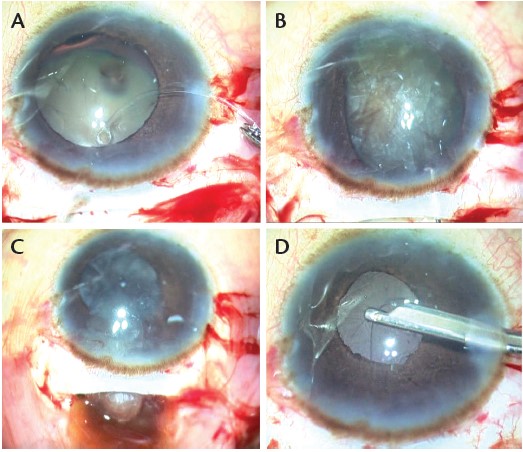
Figure 1. A patient with less than one quadrant of subluxation with dense brown nuclear sclerosis: A CTR was implanted (A), and the nucleus was dialed out (B) and then viscoexpressed through a small-incision cataract tunnel (C). Postoperatively, the patient had a well-centered IOL (D).
LESS THAN ONE QUADRANT OF SUBLUXATION
In eyes with a small degree of subluxation (one quadrant or less), I prefer to insert a normal capsular tension ring (CTR). The ring provides countertraction for all maneuvers and prevents further extension of the zonular dialysis. It also redistributes stress forces to areas of intact zonules, expands the fornix, reduces flaccidity of the posterior capsule, minimizes the risk for aspiration of the fornix or capsular bag, and decreases vitreous prolapse.
Case No. 1. A patient presented with a visually significant cataract. Clinical examination revealed a subluxation of less than one quadrant with the presence of dense brown nuclear sclerosis. Considering that in-the-bag chopping maneuvers required for disassembly of this dense nucleus would exert excessive zonular stress with resultant extension of the dialysis, small-incision extracapsular cataract surgery was planned. A large capsulorrhexis was created, and the CTR was implanted in the capsular bag. The dense nucleus was dialed out of the bag and brought into the anterior chamber. It was then brought out of the eye by viscoexpression. This was followed by in-the-bag IOL implantation (Figure 1).
WATCH IT NOW
Glued Capsular Hook Technique
Dr. Jacob demonstrates her technique of using a glued capsular hook for sutureless transscleral fixation of the capsular bag.

Case No. 2. A patient experienced intraoperative zonulodialysis during cortex aspiration. An OVD was injected into the anterior chamber before the I/A probe was withdrawn. A CTR was implanted, and this expanded the capsular bag well. The IOL was implanted in the bag with good centration and stability. The patient did well postoperatively and achieved an excellent BCVA (Figure 2).
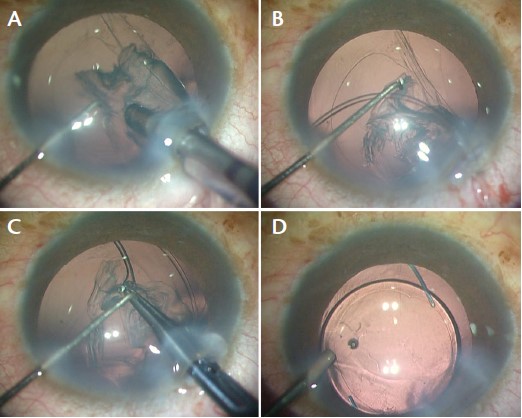
Figure 2. Zonulodialysis occurred during cortex aspiration (A). A CTR was implanted (B,C), and a well-centered IOL was achieved (D).
If dialysis is noted before nucleus emulsification, a CTR may be implanted at this time. Care should be taken to avoid all maneuvers that may increase stress on the zonules. Phaco chop may be used for nucleus disassembly. Very soft nuclei in young adults can be gently hydroprolapsed out of the bag, and the nucleus can then be safely emulsified. Cortex aspiration should be performed with care. A good cortical cleaving hydrodissection helps make subsequent cortex removal easier. Cortex entangled between the CTR and the capsular fornix should be aspirated out gently in a tangential manner using low parameters and avoiding centripetal pull on the zonules. This can then be followed by in-the-bag IOL implantation.
MORE THAN ONE QUADRANT OF SUBLUXATION
A standard CTR does not provide vertical support to the capsular bag and is not sufficient in dialysis of more than one quadrant. More than one quadrant of subluxation requires scleral fixation of the capsular bag. This can be managed with either a sutured modified CTR, such as the Cionni CTR (Morcher) and the Cionni Modified CTR (Morcher), or with a sutured capsular tension segment (CTS), such as the Ahmed CTS (Morcher) or the Assia Anchor (Hanita Lenses). My preference in these cases is to implant a CTR and then use sutureless transscleral fixation of the bag using the glued capsular hook technique, which I described in 2014.1 This is combined with CTR implantation to expand the fornix.
Case No. 3. A 59-year-old man presented with a history of injury 9 years earlier. He complained of increasing difficulty in vision of more recent onset. Examination showed a cataractous lens with subluxation of more than one quadrant. I decided to fixate the capsular bag to the sclera using the glued capsular hook technique.2 A scleral flap centered on the dialysis was created. A capsular hook was modified by changing the bend in the shaft 90° to the shaft. This was then inserted transsclerally under the iris and above the capsular bag to engage the capsulorrhexis rim.
The bag was further stabilized vertically with additional translimbal capsular hooks and horizontally with a CTR for equatorial expansion of the fornix. Phacoemulsification was carried out with in-the-bag IOL implantation. The translimbal hooks were then removed, and the transscleral hook was trimmed and tucked into an intrascleral Scharioth tunnel created at the edge of the scleral flap. The centration was adjusted by modifying the degree of tuck of the haptic into the tunnel. The flap and conjunctiva were stuck down with fibrin glue.
Postoperatively, the patient had a well-centered IOL, and BCVA improved from preoperative counting fingers to 6/9 (Figure 3).
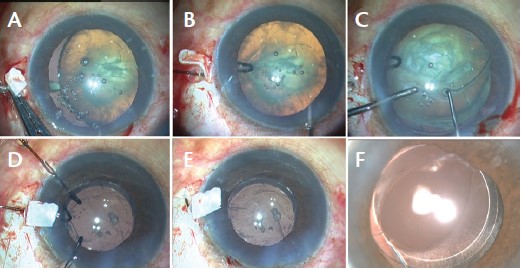
Figure 3. Glued capsular hook technique for subluxation of greater than one quadrant: A sclerotomy is made under a scleral flap centered on the area of dialysis (A). A capsular hook is used to engage the rhexis rim (B), and a CTR is implanted (C). Phacoemulsification is performed, followed by in-the-bag IOL implantation, with placement of translimbal hooks to provide additional stabilization (D). The translimbal hooks are removed, and the transscleral hook is trimmed and tucked into an intrascleral Scharioth tunnel (E). At 7 weeks postoperative, the slit-lamp photo showed a well-centered, stable IOL with the hook holding onto the capsular bag (F).
Case No. 4. Another patient presented with extensive subluxation with a dangling lens. This situation required iris or scleral fixation of the posterior chamber IOL or implantation of an anterior chamber IOL. My personal preference for dangling cataracts is to extract the cataract and implant a glued IOL3 (Figure 4). Attempting to implant a CTR in such cases can often worsen the dialysis.
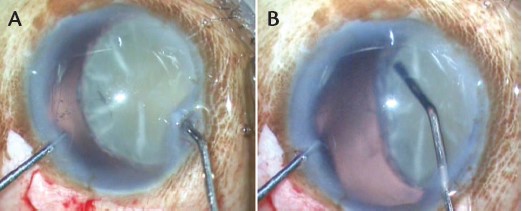
Figure 4. A dangling subluxated cataract is best managed by cataract extraction followed by glued IOL implantation (A,B).
CTR FOR SUBLUXATED IOL
The management of subluxated in-the-bag IOLs follows essentially the same decision-making process as described above and, thus, depends on the degree of zonular dialysis. The IOL can be fixed to the iris or sclera by sutures or to the sclera by sutured CTSs or with the sutureless glued capsular hook technique.
The capsular hook is attached onto the rhexis after OVD is instilled in the anterior chamber to create space between the anterior and posterior leaflets for the hook. The bag-IOL complex is anchored to the sclera using the techniques described above for subluxated cataracts. This has the advantage over sutured CTSs of not requiring a large extent of the often fibrosed bag to be opened. Separation of the leaflets is required only in an area just broad enough to insert a hook. This decreases the amount of intraoperative manipulation required.
Case No. 5. An elderly man presented with a history of trauma. On examination, a subluxated IOL was observed. The leaflets of the capsular bag were fibrosed and largely adherent to each other. A scleral flap was created centered on the area of dialysis, and a sclerotomy was created under the flap. The anterior and posterior leaflets of the capsular bag were separated over a narrow area corresponding to the sclerotomy. A modified capsular hook was inserted through the sclerotomy, and the rhexis rim was engaged with the hook. The hook was trimmed and inserted into an intrascleral Scharioth tunnel, providing sutureless fixation. The flap and conjunctiva were closed with fibrin glue. The patient had a well-centered IOL postoperatively (Figure 5).
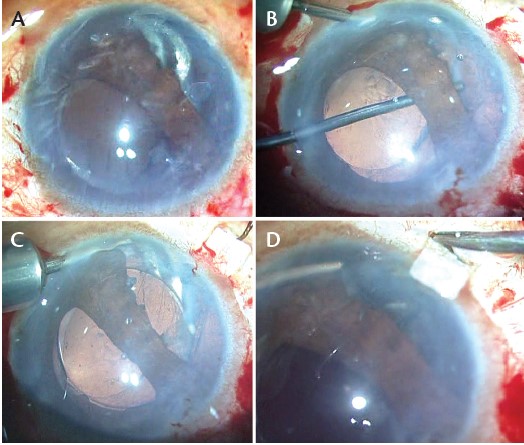
Figure 5. IOL subluxation after trauma (A). The anterior and posterior leaflets are separated in a narrow zone (B). A glued capsular hook is used to engage the rhexis (C). The haptic is trimmed and tucked, and centration is achieved by adjusting the degree of tuck (D).
Case No. 6. For intraoperative in-the-bag IOL-CTR complex subluxation, scleral fixation can be attained by passing a 9-0 polypropylene or 8-0 Gore-tex suture through the CTR and anchoring it to the sclera under a flap. A glued capsular hook technique may also be used. Large dangling subluxations may require three-point fixation or explantation followed by implantation of a transsclerally fixated glued IOL.
At a Glance
• Precautionary steps to avoid increasing subluxation can include creating a capsulorrhexis that is appropriately sized and centered; performing gentle intraocular maneuvers; avoiding intracapsular procedures that place stress on the zonules; and taking care to avoid sudden shallowing of the anterior chamber, especially while removing the phaco tip or I/A probe.
• During surgery, it is important to watch for zonular dialysis so that appropriate corrective action can be taken at the earliest indication.
• In eyes with small subluxations of one quadrant or less, a normal CTR can be inserted. More than one quadrant of subluxation requires scleral fixation of the capsular bag.
CONCLUSION
Zonular weakness presents challenges during cataract surgery. In the event of a subluxated crystalline lens or IOL, the surgeon must plan the type of surgery and the individual surgical steps with great care. n
1. Jacob S, Agarwal A, Agarwal A, et al. Glued capsular hook: technique for fibrin glue-assisted sutureless transscleral fixation of the capsular bag in subluxated cataracts and intraocular lenses. J Cataract Refract Surg. 2014;40(12):1958-1965.
2. Jacob S, Agarwal A, Agarwal A, et al. Glued endocapsular hemi-ring segment for fibrin glue-assisted sutureless transscleral fixation of the capsular bag in subluxated cataracts and intraocular lenses. J Cataract Refract Surg. 2012;38(2):193-201.
3. Kumar DA, Agarwal A, Prakash G, et al. Glued posterior chamber IOL in eyes with deficient capsular support: a retrospective analysis of 1-year post-operative outcomes. Eye (Lond). 2010;24(7):1143-1148.
Soosan Jacob, MS, FRCS, DNB
• Director and Chief, Dr. Agarwal's Refractive and Cornea Foundation (DARCF), Chennai, India
• Senior Consultant Ophthalmologist, Dr. Agarwal’s Eye Hospital and Eye Research Centre, Chennai, India
• dr_soosanj@hotmail.com
• Financial disclosure: Patent pending for modified versions of the glued capsular hook