
Ask any ophthalmic surgeon to describe the steps of cataract surgery, and he or she will likely produce a similar list of sequential steps: incision, capsulorrhexis, hydrodissection, phacoemulsification, irrigation and aspiration, IOL insertion, closure. Such a list, however, is a simplified overview, and each step, although it may be easily described, can be fraught with complexity.
AT A GLANCE
• The capsulorrhexis may be the single most important factor in a successful outcome of cataract surgery.
• To create a cauterized capsulotomy with smooth edges that would be resistant to the shear forces exacted in cataract surgery, the author conceived the idea of applying a heating element directly to the ocular tissue.
• The ApertureCTC uses thermal energy to accurately and reproducibly create a centered and round capsulotomy.
The capsulorrhexis, for example, may be the single most important factor in a successful outcome of cataract surgery: If it is centered perfectly and shaped accurately, the IOL will align with the visual axis, providing optimal conditions to achieve the desired refractive target.1-4 When capsulorrhexis creation goes wrong, however, there may be no recourse to properly position the IOL, the zonules may become weakened, and the posterior capsule may be at risk of tearing.5-8
For decades, surgeons have performed the continuous curvilinear capsulorrhexis manually. Many physiologic factors can affect its creation: the size of the pupil, globe exposure, presence of red reflex, capsule texture, consistency of the underlying lens, and other variables.
Watch it Now
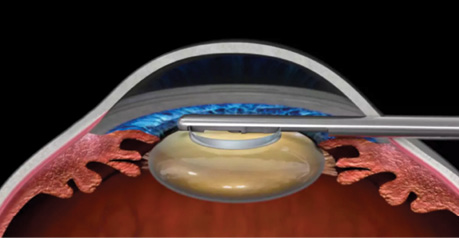
ApertureCTC Continuous Thermal Capsulotomy System
The introduction of laser-assisted cataract surgery (LACS) yielded a new option for this delicate step. Among the benefits of the femtosecond laser is its ability to precisely cut and accurately center the rhexis along the visual axis, resulting in less tilt and decentration of the IOL.9 And, yet, LACS has downsides, including the cost of these laser platforms. Another recently noted negative is that even the best laser platforms leave an edge that is less smooth than a manual capsulorrhexis edge. Electron microscopy studies have demonstrated that laser use leaves tags at the rim, with associated risk for capsular tearing.10
There is a need for an alternative approach to capsulotomy creation. In response to this need, my colleagues and I have envisioned and designed a new way of cutting the capsule using thermal energy. This device, the Aperture Continuous Thermal Capsulotomy System (ApertureCTC; International Biomedical Devices, accurately and reproducibly accomplishes the task of creating a perfectly centered and round capsulotomy. (This device is not yet cleared or approved for clinical use in Europe or the United States.)
A FORTUITOUS CONVERSATION
Many years ago, I found myself in conversation with renowned cataract surgeon Nick Mamalis, MD, of the John A. Moran Eye Institute in Salt Lake City, Utah. Dr. Mamalis remarked how difficult it was to teach the process of creating a capsulorrhexis to residents. That conversation triggered an idea in my mind, as it coincided with an ongoing project of mine: to create an entirely endocapsular technique for cataract surgery.
At the time, I had recently formed NuLens to facilitate the development of an accommodating IOL with wide accommodative amplitude, which I perceived as potentially beneficial for providing the magnification required by patients with impaired vision. I reasoned that, if phacoemulsification results in capsular fibrosis because it is not capable of completely removing the lens epithelium, and this in turn limits the mechanical ability for an IOL to restore accommodative ability, then a natural precursor to an IOL having an ability to be truly accommodative would be the existence of a surgery conducive to its success.
In my conversation with Dr. Mamalis, discussing the difficulty in performing the vitally important capsulorrhexis step in cataract surgery, and at the same time thinking about my desire to create an endocapsular cataract surgery technique, I realized that we needed a simple, easy-to-use, inexpensive device that allowed the surgeon to repeatedly cut a curvilinear capsulotomy.
Drawing on my experience and training in general ophthalmology, I focused on the idea of diathermy. I realized, however, that bipolar and radiofrequency diathermy, which are used effectively to cauterize small blood vessels, would yield rough edges when applied to the fine capsular tissue. This would result in capsular tearing at the low traction forces employed during cataract removal.
In order to create a cauterized capsulotomy with smooth edges—one that would be resistant to the shear forces the surgeon exacts during cataract surgery maneuvers—I conceived the idea of applying a heating element directly to the ocular tissue. Such an approach would avoid the unsafe use of a short circuit to burn the tissue, as in diathermy.
MAKING IT FIT
The ApertureCTC uses heat, within a low temperature range, derived from an electrical heating element that is passed through a blade 20 µm in thickness. The circular heating element is placed on the capsule over the desired capsulotomy site.
The challenge was, however, figuring out how to make a device capable of cutting a 4.5- to 6-mm capsulotomy fit through a 2-mm incision. That problem gave rise to another unique feature of this device: It is constructed with collapsing side arms that extend from the 1.2-mm primary shaft. It can be safely introduced through the primary incision and then expanded out, much like an umbrella opening up, to cut the desired round shape.
There was also the natural problem of figuring out how the blades would be attached on both sides in order to create a round shape rather than a notch-like shape. This was all part of the development process, and we eventually came up with a reliable mechanism to create the round shape that we wanted in a simple way.
THE HARD WORK OF INVENTION
Designing the ApertureCTC was a process that took 3 to 4 years. Plenty of prototypes wound up on the scrap heap. My partners and I failed time and again over that span, but, after each hiccup, I would paraphrase a favorite quote of Thomas Edison: “We haven’t failed; we have just learned another way not to do it.”
Several times, investors in this project told me to give up, to move on. Yet, after each failure, we tweaked the design and moved through a structured testing protocol that ultimately resulted in the design nearing availability for surgical use today.
SIMPLICITY AND ELEGANCE
Inventions for complex problems should be simple in design, function, and usability, and they should be applicable to as many potential situations as possible. The ApertureCTC seems to fit this description: It is elegantly designed based on fundamental scientific principles and answers a need for a simple and reproducible mechanism for cutting the capsule.
Yet the road to this invention was complex. What started with a quest to design an accommodating IOL begat a mission to invent an endocapsular cataract surgery technique, which gave rise to a need for a technique to perform a repeatable and precise capsulotomy under physiologic conditions through a minimally invasive opening.
For me, as an inventor with 48 patents for technologies used in all parts of the eye, from corneal surgery to accommodating IOLs to retinal endoscopic surgery to ophthalmic examination devices, the process of invention goes like this: You have an idea, and you apply it for the thing you developed it for, but then you look at the ramifications of the new device to figure out whether further innovation is needed, either in the device itself or a complementary invention, as well as to understand if it can be applied to other purposes.
CONCLUSION
The ApertureCTC appears to fit the definition of elegance, offering a deceptively simple solution to a complex problem. But the work is not yet done. I have an idea to apply the device for descemetomy. And once the device is approved or cleared for clinical use, other clever clinicians will no doubt add things I have never thought of to the list of applications. I look forward to that time.
1. Colvard DM, Dunn SA. Intraocular lens centration with continuous tear capsulotomy. J Cataract Refract Surg. 1990;16:312-314.
2. Ram J, Apple DJ, Peng Q, et al. Update on fixation of rigid and foldable posterior chamber intraocular lenses. Part I: elimination of fixation-induced decentration to achieve precise optical correction and visual rehabilitation. Ophthalmology. 1999;106:883-890.
3. Ram J, Pandey SK, Apple DJ, et al. Effect of in-the-bag intraocular lens fixation on the prevention of posterior capsule opacification. J Cataract Refract Surg. 2001;27:367-370.
4. Nishi O, Nishi K, Wickstrom K. Preventing lens epithelial cell migration using intraocular lenses with sharp rectangular edges. J Cataract Refract Surg. 2000;26:1543-1549.
5. Marques FF, Marques DM, Osher RH, Osher JM. Fate of anterior capsule tears during cataract surgery. J Cataract Refract Surg. 2006;32:1638-1642.
6. Muhtaseb M, Kalhoro A, Ionides A. A system for preoperative stratification of cataract patients according to risk of intraoperative complications. Br J Ophthalmol. 2004; 88:1242-1246.
7. Unal M, Yücel I, Sarici A, et al. Phacoemulsification with topical anesthesia: resident experience. J Cataract Refract Surg. 2006;32:1361-1365.
8. Olali CA, Ahmed S, Gupta M. Surgical outcome following breach rhexis. Eur J Ophthalmol. 2007;17:565-570.
9. Friedman NJ, Palanker DV, Schuele G, et al. Femtosecond laser capsulotomy. J Cataract Refract Surg. 2011; 37:1189-1198.
10. Bala C, Xia Y, Meades K. Electron microscopy of laser capsulotomy edge: interplatform comparison. J Cataract Refract Surg. 2014;40:1382-1389.
Joshua Ben-Nun, MD
• Consultant to IBMD
• jbnot1@hotmail.com
• Financial disclosure: Consultant (IBMD)