

Ophthalmology is a technology-heavy field. From diagnostic tools and imaging, to ultrasound and laser, to treatment with implantable devices, ophthalmologists utilize technology at almost every step. Like many ophthalmologists today, I am a pretty high-tech guy. I am used to carrying an iPhone and having ready access to all manner of apps and maps—in my car, at home, wherever I am.
In the OR and during surgery, however, being faced with analog microscopes made me feel like I was stepping back in time 10 years. The microscope was still lacking the ability to provide digital guidance and data directly to the surgeon during procedures. I could not help wonder, “Why does the technology in the OR involve me printing out a piece of paper and taping it to the microscope I am using?”
AT A GLANCE
• The challenge for the physician-inventor is not just generating an idea but also understanding how to get from an idea to a commercially viable product.
• The Cirle medical technology incubator has a comprehensive process in place, including research and development, prototyping, software and hardware engineering, quality assurance, and regulatory review.
• The Cirle/Spectrus Surgical Navigation System is the first to offer 3-D graphics that are viewable directly in the microscope.
From there, my question became, “What if we could visualize imaging and annotations while looking in the microscope?” That was my initial brainstorm, leading me to the goal of achieving digitally assisted cataract surgery.
THE POWER OF INTUITION
The best piece of technology works seamlessly in the user’s life: He or she uses it but does not have to change his or her life or behavior in order to do so. Like an iPhone, it is intuitive.
To make a technology successful in the OR, it too must be intuitive. It must think like a surgeon, so, ideally, it is developed by a surgeon from day 1. In fact, the most successful medical technology, both in and out of the OR, has incorporated physician feedback early in the process.
As an example of what I consider unsuccessful medical technology, take electronic health records. Many ophthalmologists have great disdain for these systems. A closer look into the development of electronic health records reveals that doctors were brought in at the last minute.
As a surgeon, my experience and intuition help mold my expectations for a tool to work a certain way. Through Cirle, the medical technology incubator I founded in 2010, my goal is to develop products that grow around that impulse.
THE PATH OF INVENTION
It took quite a while to get from having an idea in my head to figuring out how it could become reality, and many things happened along the way. The product development process can be oversimplified into two steps: (1) the practitioner identifies an unmet need and (2) the practitioner works with industry to make that idea a reality. But it goes beyond that.
Between the starting point of having no intraoperative guidance and achieving the ultimate digital solution, there is an infinite number of ways to fail. However, simply moving from zero (no idea) to one (the first concept) is the hardest part. At that early point, there are a million people to tell the physician-inventor what is wrong with his or her idea and why it will not be successful.
A crucial piece for me was to believe in the future and in where things could possibly go. I also needed to listen to the positive ideas of others. I surrounded myself with people who believed in and were enablers for the project. Listening to their credentialed and vetted feedback was key. In particular, I credit my surgical and ophthalmic colleagues at Bascom Palmer Eye Institute for their excellent medical perspectives.
The other critical piece is having a strong team of people; this includes surrounding oneself with great team members and great industry partners throughout the process. All of those individuals helped to balance the idea of a surgeon’s unmet need with what could be commercially viable. A product must be important to doctors as well as workable in the marketplace in order to be successful. I cannot underscore enough how important our commercial and industry partners have been in the process, as well as mentoring and developing our internal team talent.
INCUBATING MEDICAL TECHNOLOGY
My path to invention is partly fueled by my background in academic medicine, but importantly driven by asking questions, both in the clinic and the OR. Why do we do things in certain ways? How can we do them better? What would I want if I were the patient?

Figure 1. The Cirle Surgical Navigation System.
The challenge for the physician-inventor is not just generating an idea but also understanding how to get from an idea to a commercially viable product. Understandably, industry experts prefer to receive ideas that are advanced enough for them to run with; however, it is often challenging for doctors to deliver something in that state. Another aspect is surrounding oneself with people who know things better than that individual—and I credit our internal team at Cirle and external industry partners with driving that forward.
At Cirle, we have a comprehensive process in place, including development, quality assurance, supply chain management, and regulatory review. Over the past several years, we have been building an experienced research and development team of program managers, hardware and software
engineers, and regulatory and quality experts to execute these tasks.
The first output of the team is the Cirle Surgical Navigation System, which Bausch + Lomb has licensed and will market under the name Spectrus (Figure 1).
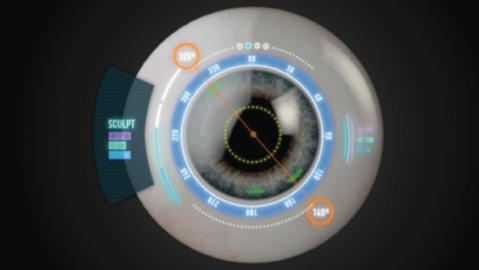
Figure 2. 3-D overlays are viewable directly in the microscope.
This system is the first to offer 3-D graphics (Figure 2) that are viewable directly in the microscope. Markings for incisions are seen on the cornea, capsulorrhexis guidance is projected at the level of the anterior capsule, and lens alignment marks are visible at the IOL level. The images are in remarkable full color and are a product of our proprietary Holotagging image guides and StereoCapture image-acquisition technology.
These graphics assist the surgeon at a number of crucial points, including preoperative planning, alignment, and placement of astigmatic toric IOLs; incision guidance for primary and secondary incisions; capsulorrhexis creation; monitoring phaco parameters; and delivering intraoperative ultrasound, vacuum, and irrigation.
Our overarching goals are improved workflow and efficiency and, ultimately, patient satisfaction. To that end, using the Cirle system does not require any change in the surgeon’s preferred technique, and the learning curve is minimal.
LOOKING FORWARD
The intersection of technology and health care is such an exciting place to work in, and, ophthalmology—from clinical practice to the OR—is a medical field that is technology-intense, and it will continue to benefit from technologic innovation, whether through device innovation or software development. I see the navigation system as a platform technology with a great deal of potential.
Richard M. Awdeh, MD
• Professor, Surgeon, and Director of Technology Transfer, Bascom Palmer Eye Institute, Miami
• Founder and CEO of CheckedUp and Cirle
• richard@cirle.com
• Financial disclosure: Founder (Cirle medical technology incuba- tor), Inventor (Cirle/Spectrus Surgical Navigation System)