
Today, patients living with disability from retinal disease cope with activities of daily living through the use of electronic devices or monocular fixed focus intraocular telescopes to magnify the image on the retina.1 These devices, however, have significant limitations. External devices may be cumbersome and expensive, and they may not be available to the patient at all times and in all places. Intraocular telescopes are difficult to implant, costly, and offer only a restricted field of view with a fixed focus. The monocular image magnification with the telescope commonly causes patient confusion from the associated anisoconia.
AT A GLANCE
DESIGN CRITERIA OF THE CONEXUS LENS
• Actuation by less than 1 g of axial force and less than 200 μm of movement
• Accommodative amplitude of 10.00 D with maximum image quality as measured by visual Strehl ratio throughout the accommodative range (3X to 6X retinal image magnification)
• Control by the eye’s natural positive autonomic feedback system
• Ability to pass through a small, sutureless (< 3 mm) incision
• Minimal refractive discontinuities in the lens optic to minimize scatter and maximize image quality throughout the accommodative range
• Field of view equivalent to a monofocal IOL
• Ability to utilize pupillary miosis during actuation for near focus
• Dimensions of 5.5 to 6.5 mm optic diameter and 2.5 mm maximum thickness utilizing existing biocompatible lens material
• Continued operation and stability after implantation with dynamic resistance to cellular ingrowth and disengagable anterior lens
• Ability to operate despite Nd:YAG capsulotomy and capsular phimosis, with registering haptics that reset to zero actuation
• Simplicity and low price compared with existing technologies under development
Intuor Technologies is developing a variable hyperfocal IOL to be implanted at the time of cataract surgery, the Conexus Lens, that is designed to aid mild to moderate age-related macular degeneration (AMD) patients.2 This technology should be transferable upon regulatory approval, in an attenuated version, to an accommodating IOL. The company demonstrated the conceptual feasibility of the Conexus Lens approach through mechanical and optical modeling, and created a preliminary prototype using coupled existing lenses (see The Conexus Lens).
THE CONEXUS LENS
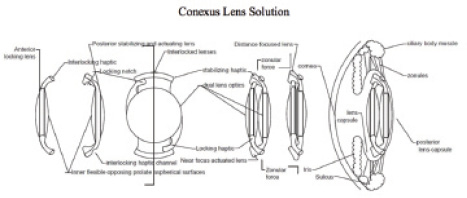
In this image, the hyperfocal applanating variable focus IOL is shown in its individual components (left), assembled (center), and in its intraocular configuration (right). In bench testing, the preliminary prototype lens:
• Produced greater than 16.00 D of lens power change with good optical image quality (visual Strehl ratio greater than 0.7);
• Required less than 1 g of axial force for actuation; and
• Maintained a greater than 120° full field of view.
Our design approach is simple, and it provides the ophthalmic surgeon a valuable alternative for AMD patients retaining some macular function in need of cataract surgery. Implantation of the Conexus Lens varies only minimally from standard cataract surgery. Currently, for AMD patients, most ophthalmologists will implant a fixed-focus lens and set the patient’s refraction to approximately 3.00 D to maximize image magnification on the retina. After surgery, the patient will still require use of expensive external low-vision aids such as video electronic systems. A few ophthalmologists are capable of the more surgically complex and expensive implantation of monocular telescopes, such as the Implantable Miniature Telescope (VisionCare Ophthalmic Technologies). Retinal and cortical cerebral stimulators for usable vision appear far from routine commercial deployment at this point.
Changing power inside the eye with a COUPLED LENS DESIGN
In contrast, the Conexus Lens changes the power inside the eye to allow the patient’s associated focal distance to vary at will by more than 12.00 D. The lens enables a patient to focus at 2 inches, as opposed to a normal 25-year-old who cannot focus any closer than 15 inches. This represents a 6X increase in magnification, allowing the image to subtend a 36X greater area of the retina, utilizing the nondiseased portions of the retina to greatly improve visual acuity. The patient can then read and write at close distances and can see maximally at distance with a normal full field of view.
The design of the Conexus Lens is a mechanically coupled lens system with deforming applanating surfaces (Figure 1). During surgery, each lens will be inserted individually through a sub–3-mm incision and then coupled inside the eye. Optimization of the design is being completed according to our published methodology.3
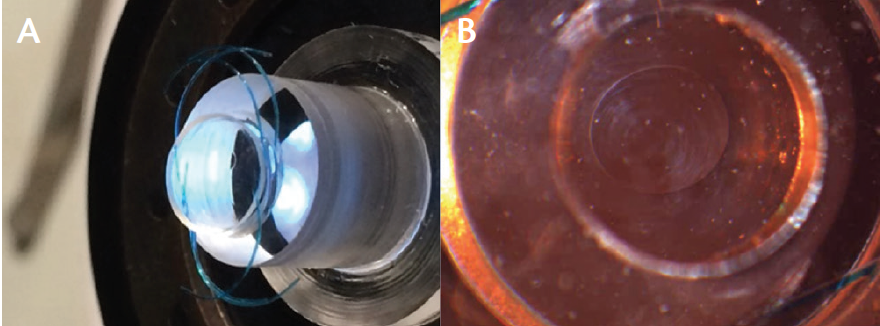
Figure 1. Proof of concept: Disassembled piston/cylinder with stacked off-the-shelf silicone lens implants with a 6 mm diameter (A) and a retroilluminated microscopic image of the applanating interface (B).

Figure 2. Images taken through the preliminary prototype showing 16.00 D of power change (in air) using 0.7 g of axial force.
Applanation of the interface progressively negates the contribution of refractive power in the Conexus Lens system, in direct proportion to the amount of physiologic accommodating force applied. The coupled accommodating IOL is positioned in the capsular bag, and soft foldable haptics conform it to the native shape of the lens, utilizing an open capsule concept.
The mode of actuation of the lens system is provided by the natural mechanism by which the native lens accommodates, and the force is modulated by the natural autonomic feedback system to adjust the force to the amount of accommodation needed. The annular ciliary body muscle contracts during near accommodation, reducing the tension on the radially positioned zonules. The zonular relaxation reduces both radial tension and axial compression, releases any applied force to the accommodating IOL, and the IOL resumes its unstressed/undeformed state in which it is focused for near vision. Conversely, with ciliary muscle relaxation, the zonular tension is increased, which creates a radial expansion and a coupled axial compression through mechanical coupling of the lens system. The coupled axial compression actuates the IOL for distance vision focus.
PROTOTYPE PERFORMANCE
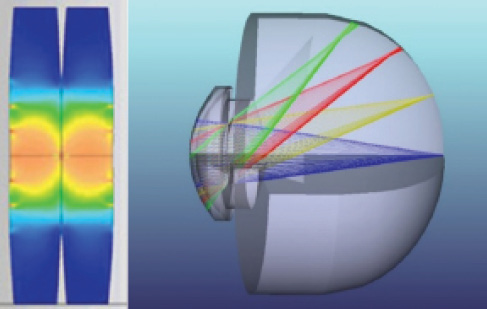
Figure 3. Preliminary mechanical finite element model and associated optical ray-trace model.3
A preliminary prototype coupled deforming lens was built using commercially available silicone IOLs. This prototype demonstrated the ability to obtain an extraordinary change in power with less than 1 g of pressure (Figure 2), which is well within the physiologic force available in the human eye to accommodate the natural lens (Figure 3).
The Conexus Lens design addresses the difficult challenges inherent to accommodating IOLs. Conexus’ implantable prototype will demonstrate the design criteria described in At a Glance.
CONCLUSION
The simplicity of the Conexus Lens design and its coupled actuation maximizes the probability of an effective IOL implant. Our lens will work within the constraints of the human eye with regard to available physiologic actuation force, neurologic control, space limitations, biocompatibility, and long-term operation.
1. Picaud S, Zrenner E, Pezaris J, et al. Chapter 7 – Restoring vision to the blind: advancements in vision aids for the visually impaired. Transl Vis Sci Technol. 2014;3(7):9.
2. McCafferty S. Variable hyper-focal IOL design to aid macular degeneration patients. Paper presented at: American Society of Cataract and Refractive Surgery Annual Meeting; April 21, 2015; San Diego.
3. McCafferty SJ, Schwiegerling JT. Deformable surface accommodating intraocular lens: second generation prototype design methodology and testing. Transl Vis Sci Technol. 2015;4(2):17.
Sean McCafferty, MD, FACS
• CEO/President, Intuor Technologies, Tucson, Arizona
• sjmccaff@conexuslens.com
• Financial disclosure: Employee/President and CEO (Intuor Technologies)