

The availability of femtosecond lasers for use in some aspects of cataract surgery has grown significantly over the past few years, and a large percentage of cataract surgeons now have access to the technology. Laser-assisted cataract surgery (LACS) has the potential to help reduce complications and improve visual outcomes, and further innovations will help surgeons achieve these goals. One of the keys for success with any technology is identifying which patients are appropriate candidates for its use and which are not.
AT A GLANCE
• Although achieving good dilation is ideal for any form of cataract surgery, patients who do not dilate well can still be candidates for LACS.
• In many eyes with small pupils, after the femtosecond laser portion of the procedure, a Malyugin Ring can be placed to expand the pupil size and make the rest of the procedure easier.
One requirement for LACS is the ability to dilate the patient’s pupil, as the laser can treat only the portion of the cataract that is visible through the pupil. With any poorly dilated pupil, the laser will not be able to visualize or treat the cataract. By contrast, a well-dilated pupil allows the laser to visualize the cataract, perform a centered capsulotomy, and properly fragment the nucleus of the lens.
IDEAL SIZE AND ALTERNATIVES
There is some debate over the optimal size for the capsulotomy. Many surgeons prefer a capsulotomy diameter in the range of 4.8 mm, which allows maximal overlap of the anterior capsule with the optic of the IOL. Recent research by Packer and colleagues suggests that the optimal diameter for laser capsulotomy should be 5.25 mm, as this size provides the strongest capsulotomy and thereby helps avoid capsular tears.1 This larger capsulotomy size offers an improved surgical experience and still provides reasonable capsular overlap of the IOL optic.
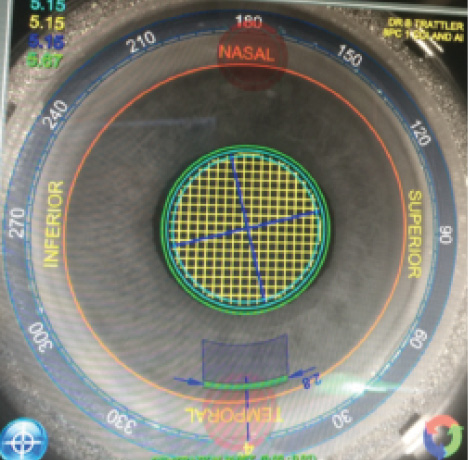
Figure 1. The LACS planning overlay on the Lensar laser. Note the temporal 2.8-mm clear corneal incision (green), the capsulotomy outline (orange), and laser fragmentation pattern (center), as planned in an eye with a small pupil.
Although the ideal capsultomy size may be greater than 5 mm, there is a percentage of patients whose pupils, even with dilating drops, will allow room only for a capsulotomy of less than 5 mm. If LACS is the preferred modality for capsulotomy creation, the question is: How small a capsulotomy is reasonable?
First let us acknowledge that there are alternatives to laser capsulotomy when a small pupil is encountered. Some surgeons prefer to perform standard cataract surgery with insertion of a Malyugin Ring (MicroSurgical Technology) or iris hooks, creating a manual capsulotomy in the range of 5 mm diameter. Another approach, preferred by some surgeons who feel that the femtosecond laser portion of cataract surgery is crucial to the success of the procedure, is to first initiate cataract surgery, creating the paracentesis and primary incision. After this, a Malyugin Ring is placed, and only then is the patient taken to the femtosecond laser. Although this sequence can be used, there are challenges with this approach, especially if the femtosecond laser is not in the operating room.
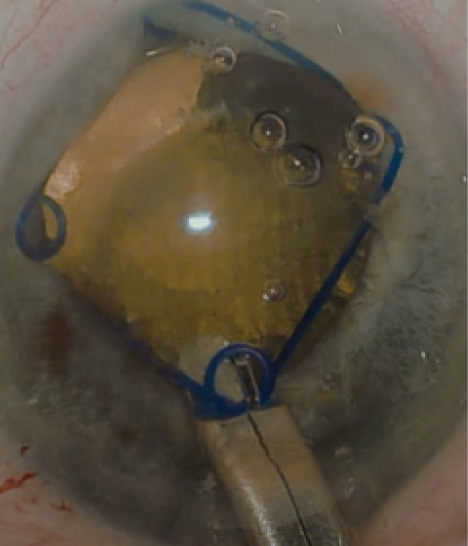
Figure 2. Malyugin Ring placed after femtosecond laser caspulotomy.
OUTCOMES STUDY AND IMPLICATIONS
With these issues in mind, our center evaluated the outcomes of LACS in patients who had pupil sizes of less than 6 mm diameter at the time of surgery (Figure 1). This study included 32 consecutive patients (13 women and 19 men) whose mean age was 76 ±8.3 years. The mean pupil size was 5.2 ±0.24 mm, and the mean capsulotomy size was 4.7 ±0.3 mm (range, 4.1–5 mm). The smallest capsulotomy size in this evaluation was 4.1 mm, which is just 0.1 mm larger than the smallest size allowed by the Lensar Laser System (Lensar). After capsulotomy creation and nuclear fragmentation, all patients underwent successful cataract surgery with no complications.
Although our clinical study of patients with small pupils undergoing LACS had a small sample size, its results have been borne out by my experience since the study was completed. That is, even with small capsulotomy sizes between 4.1 and 4.5 mm, LACS procedures can proceed smoothly.
In many eyes with small pupils, after the femtosecond laser portion of the procedure, I place a Malyugin Ring to expand the pupil size and make the rest of the procedure easier (Figure 2). Other interventions, including administering preoperative NSAIDs, Omidria (phenylephrine and ketorolac injection; Omeros), and/or Shugarcaine (epinephrine and lidocaine in balanced salt solution),2 may also be efficacious in patients who do not dilate well at the time of cataract surgery.
SUMMARY
Although achieving good dilation is ideal for any form of cataract surgery, patients who do not dilate well can still be candidates for LACS. The smallest capsulotomy size evaluated in our study was 4.1 mm, and these cases were performed without complication. I do not have experience with capsulotomies smaller than 4.1 mm or experience with surgical dilation of the pupil with a Malyugin Ring prior to performing the femtosecond laser steps of LACS.
1. Packer M, Teuma EV, Glasser A, Bott S. Defining the ideal femtosecond laser capsulotomy. Br J Ophthalmol. 2015;99(8):1137-1142.
2. Myers WG, Shugar JK. Optimizing the intracameral dilation regimen for cataract surgery: prospective randomized comparison of 2 solutions. J Cataract Refract Surg. 2009;35(2):273-276.
William B. Trattler, MD
• Director of Cornea, Center for Excellence in Eye Care, Miami, Florida
• wtrattler@earthlink.net
• Financial disclosure: Consultant (Lensar)