


Many refractive surgeons have adopted femtosecond laser technology for creating LASIK flaps. In our practice, we have embraced this technology, and we no longer even have a mechanical microkeratome.
AT A GLANCE
• Detailed preoperative assessment in post-RK patients includes OCT imaging of the cornea in order to determine two important variables: the total central corneal pachymetry and the average central corneal epithelial thickness.
• Use of a thicker target flap depth in post-RK eyes confers increased structural integrity to the flap, which already contains multiple radial incisions and less stroma on average due to the thickened epithelium.
• When femto-LASIK is performed in these eyes, it is necessary to increase laser power settings accordingly to cut a flap that contains no or almost no stromal tissue bridges, especially at the site of the RK incisions.
We encounter many middle-aged adults who had RK while in their 20s in the early 1990s. Many of these patients now seek additional refractive treatment options because they have developed hyperopic regression that is becoming more noticeable and bothersome, especially as they become increasingly presbyopic. To address these issues, surgeons may choose to offer such patients surface ablation, refractive lensectomy, or even LASIK. Successful use of microkeratome techniques has been described in this setting.1 There is, however, limited experience regarding femtosecond LASIK (femto-LASIK) techniques in these patients.
Several intra- and postoperative complications have been encountered using the femtosecond laser after previous RK, including loss of suction, opening of RK incisions by vertical gas breakthrough, epithelial ingrowth, and flap interface inflammation and haze.2 In this article, we describe our technique to perform femto-LASIK successfully after RK.3,4
PREOPerative ASSESSMENT
Detailed preoperative assessment in these patients includes OCT imaging of the cornea in order to determine two important variables: the total central corneal pachymetry and the average central corneal epithelial thickness. Notably, post-RK patients have not only thicker total corneal pachymetry than average but also thicker epithelium. This information is important to consider in determining the appropriate target flap depth.
For example, we have encountered a post-RK patient who had a baseline central corneal epithelial thickness of 100 µm. Obviously, in this scenario, our standard target flap depth (110 µm) would be inadequate and would likely result in an unstable flap. Trying to surgically manipulate a flap containing so little stroma would also likely lead to spreading of the RK incisions.
Estimated residual stromal tissue is not a significant issue in this setting because corneas are typically thicker and ablation profiles are usually hyperopic. Therefore, we generally select target flap depths of around 160 to 200 µm. The thicker target flap depth confers increased structural integrity to the flap, which already contains multiple radial incisions and less stroma on average due to the thickened epithelium. The enhanced thickness is a benefit when the surgeon is attempting to lift and retract the flap during surgery.
SETTINGS
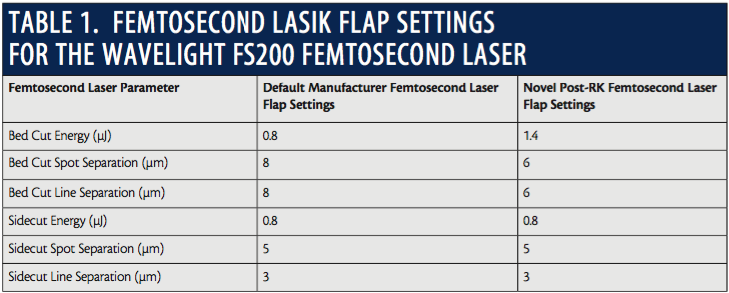
Femtosecond laser settings are crucial components of success. We find that the standard default manufacturer settings on our platform (WaveLight FS200; Alcon) leave too many stromal tissue bridges to be separated on a flap that is already structurally compromised.
Although histologic studies have shown absence of stromal fibrosis around the areas of RK incisions,5 in clinical practice we find that the RK incisions may be considerably more adherent to the underlying stromal bed than the normal adjacent surrounding tissue when standard femtosecond laser settings are used. In this scenario, the surgeon faces a risk of unzipping an RK incision when trying to release the stromal tissue bridges and lift the flap at the site of these incisions.
Therefore, it is necessary to increase power settings accordingly to cut a flap that contains no or almost no stromal tissue bridges whatsoever, especially at the site of the RK incisions. As a further benefit of these enhanced flap settings, when the stromal bed visibly separates at the same time that the femtosecond flap cut occurs, no opaque bubble layer (OBL) forms because the gas collects in the newly created potential space in the flap interface. This helps prevent excessive OBL formation and trapping of gas bubbles that can create vertical breakthrough and opening of a weakened RK incision.
Our novel post-RK settings are detailed in Table 1 and compared with the standard default manufacturer femtosecond laser flap settings. It is important to be mindful that increasing energy and spot size will cut a flap that may be thinner than anticipated, approximately 10 µm thinner than expected with our settings.
LIFTING THE FLAP
Since our femtosecond laser settings will create a flap that may contain no connective stromal tissue bridges, less manipulation of the flap is needed, and less trauma is induced when it is retracted. We start by inserting a blunt-tipped LASIK flap retractor at just one location between two RK incisions. The instrument is immediately advanced centrally to ensure that there are no flap adhesions in the central optic zone that contains no RK incisions.
Then, before the blunt-tipped instrument is retracted, slow and gentle sweeping movements are made from the center to the periphery, releasing the entire flap from any remaining adhesions. We believe that starting peripherally and working centrally is more traumatic and would be more likely to result in an undesirable opening of an RK incision.
LASER TREATMENT
Once the flap is safely retracted, the excimer laser treatment and flap repositioning portions of the procedure are continued using standard techniques. Lining up the repositioned flap with the peripherally extending RK incisions may even assist the surgeon with flap realignment. We typically do not place a bandage contact lens.
We also caution that no attempt should be made to continue the treatment if an opening of an RK incision is encountered at any point, whether at the time of femtosecond laser treatment or at the time of flap lifting and retraction. We believe this would be a significant risk factor for subsequent development of postoperative epithelial ingrowth and postoperative refractive instability with unpredictable outcomes.
SUMMARY
We have described a technique to safely and reliably perform femto-LASIK in the setting of previous RK. Our long-term visual outcomes using this technique have been comparable to LASIK outcomes on age-matched eyes without a history of RK.3,4
We have not used this technique in patients with more than an eight-incision RK pattern, and we have not studied the technique prospectively. We believe that this technique adds an extra option for the refractive surgeon confronted with these complex cases, but we caution that each case must be individually evaluated to determine the optimal type of procedure and the specific treatment technique to be offered to the patient.
1. Francesconi CM, Nose RA, Nose W. Hyperopic laser-assisted in situ keratomileusis for radial keratotomy induced hyperopia. Ophthalmology. 2002;109:602-605.
2. Perente I, Utine CA, Cakir H, et al. Complicated flap creation with femtosecond laser after radial keratotomy. Cornea. 2007;26:1138-1140.
3. Rush SW, Rush RB. One-year outcomes of femtosecond laser-assisted LASIK following previous radial keratotomy.
J Refract Surg. 2016;32(1):15-19.
4. Rush SW, Rush RB. Femtosecond laser flap creation for laser in situ keratomileusis in the setting of previous radial keratotomy. Asia Pacific J Ophthalmol. 2015;4(5):283-285.
5. Bergmanson J, Farmer E, Goosey J. Epithelial plugs in radial keratotomy: the origin of incisional keratitis? Cornea. 2001;20(8):866-872.
Ryan B. Rush, MD
• Partner, Panhandle Eye Group, Amarillo, Texas
• Assistant Clinical Professor, Texas Tech University Health Sciences Center, Amarillo, Texas
• Private practice, Southwest Retina Specialists, Amarillo, Texas
• ryanbradfordrush21@hotmail.com
• Financial disclosure: None
Sloan W. Rush, MD
• Partner, Panhandle Eye Group, Amarillo, Texas
• Assistant Clinical Professor, Texas Tech University Health Sciences Center, Amarillo, Texas
• Sloan.rush@paneye.com
• Financial disclosure: None