

Keratoconus is a conic corneal dystrophy, mostly in the inferior part of the cornea, that causes irregular astigmatism and can lead to visual impairment that cannot be properly corrected with glasses. One in 2,000 individuals has keratoconus, and the incidence is higher in Arabic countries. The evolution of keratoconus is characterized by rapid progression in young patients and a tendency to stabilize with age. In some cases, the progressive protrusion of keratoconus suddenly and spontaneously stabilizes, a condition known as forme fruste keratoconus.
AT A GLANCE
• The two priorities in keratoconus management are determining whether CXL can be performed and then selecting an approach for visual rehabilitation—first contact lenses, then surgery.
• Mini scleral contact lenses are comfortable for patients, often enabling full-day wear, and they present no risk of corneal scarring.
• If mini scleral contact lenses are not an appropriate solution, surgical techniques can be employed for visual rehabilitation.
Previously, there were only two (imperfect) treatment options for keratoconus: (1) rigid contact lenses, which cause irritation and scarring, and (2) in patients with contact lens intolerance and major deformation, penetrating keratoplasty, which comes with the risk of graft rejection.
Since 2005, however, it is has been possible to stabilize the irregular deformation of the cornea by crosslinking its collagen fibers. After application of vitamin B2 (riboflavin), the cornea is exposed to UV-A light; this creates additional bonds between the collagen fibers of the cornea, which enhances the rigidity of the cornea and stabilizes the conus. CXL is indicated (1) for patients younger than 20 with keratoconus and (2) for patients with proven progression of keratoconus, confirmed, for example, by comparison of anterior topographic maps of the cornea over time.
Once keratoconus has been stabilized, whether after CXL or through the natural aging process, a visual rehabilitation strategy can be considered. In the past, the norm was to prescribe rigid contact lenses; however, many patients were intolerant of them or developed scarring due to friction with the contact lens.
MINI SCLERAL CONTACT LENSES
Treatment options have since evolved to include mini scleral contact lenses (Figure 1). In terms of visual quality, the results with these lenses are comparable to those with rigid contact lenses. Patient comfort, however, is much greater, and full-day wear is often possible. Further, because the lens is not in contact with the conus, there is no risk of corneal scarring.
Figure 1. A mini scleral contact lens.
Mini scleral contact lenses have been implemented by a limited number of centers in Belgium. In my opinion, not enough attention is paid to the nonsurgical visual rehabilitation of keratoconus patients who adopt these lenses. This is only possible if surgeons are teamed up with experienced optometrists. We have formed such partnerships in my practice with increasing success over the past 3 years.
Since adopting mini scleral contact lenses in 2011, I have observed an impact on my surgical volume in patients with keratoconus. Comparing two 3-year periods, 2007 to 2010 and 2011 to 2014 (when we started using mini scleral contact lenses), I found that my surgical numbers dropped dramatically: intrastromal corneal ring segment (ICRS) implantations were down by 81%, topography (topo)-guided PRK by 80%, and phakic IOL implantation by 60%.
ALTERNATIVES TO MINI SCLERAL CONTACT LENSES
If mini scleral contact lens adoption is not the appropriate solution for some patients, there remain three surgical techniques for visual rehabilitation that aim to recenter the conus and diminish corneal irregularity, ametropia, and irregular astigmatism. These include: topo-guided excimer laser surface treatment (PRK), implantation of a toric phakic IOL such as the Artisan or Artiflex (Ophtec), or ICRS implantation. The choice of any of these techniques depends on patient parameters.
These surgical techniques should be used only for contact lens–intolerant patients, as the quality of vision obtained with contact lenses will always be higher than that obtained with any surgical technique. The surgeon’s aim is to obtain visual rehabilitation and make the patient more functional—not to achieve emmetropia. Often the vision in the operated eye will be sufficient for the patient not to be constantly dependent on his or her glasses or contact lenses.
NO CONSENSUS
I organize an annual experts’ meeting on the surgical management of patients with keratoconus. The aims of this meeting include reaching consensus on the management of keratoconus and our surgical treatment options and sharing pearls with less experienced surgeons. We have held seven Current Surgical Options in the Management of Keratoconus meetings since 2010. Each year, I observe that, among the experts, there is a clear division into two opposing schools, with the supporters of excimer laser rehabilitation techniques on one side and the supporters of ICRS implantation on the other.
Each group successfully defends and applies its preferred technique; there is no agreement on parameters to determine when laser techniques are best indicated or when ICRSs are the adequate solution. A substantial amount of work still must be done to evaluate each keratoconus case individually and determine the best rehabilitation technique. In my observations, surgeons also tend to forget that we can obtain excellent results with phakic IOLs, especially when the conus is centered and ametropia and cylinder are high.
THREE SURGICAL APPROACHES
In my center, I employ all three techniques—topo-guided PRK, ICRSs, and phakic IOLs—and I sometimes choose to combine several of them to achieve the best possible outcome. My treatment decision is based on several parameters, such as spherical equivalent, astigmatism, corneal thickness, aspect of the conus, and BCVA. I aim for near emmetropia.
Topo-guided surface ablation. Topo-guided surface ablation (Figure 2) can be performed after or in combination with CXL. This procedure is irreversible, and most surgeons agree that the ablation should not exceed 50 µm, which implies that a limited amount of spherical equivalent or astigmatism can be corrected. The possibility of retreatment is limited because there is not enough residual tissue available. In my experience, there are also more side effects with topo-guided surface ablation, often because the treated eye is in greater competition with the better, untreated eye.
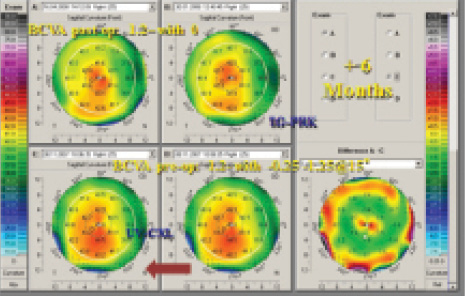
Figure 2. Topographic maps of a patient treated with CXL and topography-guided PRK.
Advantages of this technique are that the conus is recentered and the cornea is made more regular. In my practice, I favor topo-guided PRK for patients with lower degrees of ametropia. Topo-guided PRK can also be used in a second stage as a fine-tuning tool if needed after phakic IOL implantation.
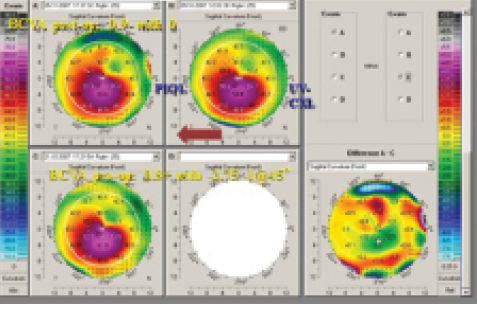
Figure 3. Topographic maps of a patient treated with CXL and phakic IOL implantation.
Phakic IOL implantation. With phakic IOL implantation (Figure 3), previous CXL is mandatory in cases of progressive keratoconus and in young patients. Advantages of this approach include that the treatment is theoretically reversible and that high myopia and astigmatism (up to -7.50 D) can be corrected. The refractive outcome is predictable, and there are almost no side effects. Disadvantages are that the cornea remains unchanged and that an intraocular technique involves more risks than a surface procedure.
A phakic IOL is best indicated in patients with a centered conus and good BCVA. Patients tend to achieve greater postoperative independence from glasses or contact lenses compared with other surgical visual rehabilitation techniques, and, surprisingly, a higher satisfaction rate is seen, mostly due to the correction of high ametropias. I have a slight preference for phakic IOLs in patients with higher ametropias.
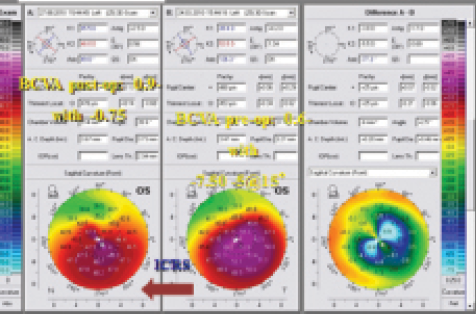
Figure 4. Topographic maps of a patient treated with CXL and ICRS implantation.
ICRS implantation. ICRS implantation (Figure 4) may not require previous CXL, even in eyes with progressive keratoconus or in young patients. Some surgeons claim that ICRS implantation stabilizes keratoconus, but this remains controversial. Advantages of this technique are its reversibility, the ability to recenter the conus, the regularization of the cornea, and the ability to correct higher myopia and astigmatism.
ICRSs are best indicated in patients with a decentered conus and slightly lower BCVA. Halos are a side effect, but they are reported by patients to be not too disturbing, and patient satisfaction rates are acceptable. In my experience, I find the results of ICRS implantations to be less predictable, although this technique sometimes yields surprisingly good results.
Combination. A combination of all of these techniques is also possible.
LAST OPTIONS
The evolution of keratoconus management has made corneal grafts increasingly redundant. If a corneal graft is the only solution, the preference should be for anterior lamellar grafts (ie, deep anterior lamellar keratoplasty), in which only the anterior layers of the cornea (epithelium and stroma) are replaced, instead of penetrating keratoplasty, in which the total thickness of the cornea is replaced.
Advantages of anterior lamellar techniques include greater patient comfort, faster healing, a less fragile eye postoperatively, and greater predictability of visual results.
Jérôme C. Vryghem, MD
• Medical Director, Brussels Eye Doctors, Belgium
• Member, CRST Europe Editorial Board
• info@vryghem.be
• Financial interest: None acknowledged