


Case Presentation

A colleague of mine, a 64-year-old obstetrician-gynecologist, underwent laser-assisted cataract surgery (LACS) with bilateral implantation of a multifocal IOL at another institution. He then had laser astigmatic keratotomy (AK) to correct residual astigmatism in his right eye; inadvertently, one of the AKs was placed near the visual axis. The patient was extremely unhappy with this result. In his right eye, UDVA was 20/80 with poor vision, and CDVA was 20/50.
Figure 1 shows the offset AKs in two images. One incision is only about 2.6 mm from the visual axis, and the paired AK is at the limbus. Anterior segment OCT (Figure 1A) shows how deep the central AK was, about 95% of corneal thickness; it would have been a perfect AK if placed correctly.
Figure 2 shows the Placido disc–derived topography, with significant irregular astigmatism, and biometry data showed his axial length as more than 26 mm. This led me to believe that he probably was about a -6.00 D myope before the surgery.
The OCT epithelial maps (Figure 3) also showed some irregularity; the blue areas correspond to the limbal AK incision. Pupillometry demonstrated a relatively moderate pupil size.
Contestants, please comment on the following:
- What would you do to address this patient’s poor result and make him happier?
- What would you have done as the secondary intervention for this patient—a myopic physician in his mid-60s who had multifocal IOLs implanted at cataract surgery and experienced a residual astigmatic refractive error?
- If this patient presented for cataract surgery, would you choose a toric presbyopia-correcting IOL for the primary intervention? I ask this because the Trulign Toric IOL (Bausch + Lomb), the Symfony Toric IOL (Abbott), and the Restor Toric IOL (Alcon) are toric presbyopia-correcting IOLs available to our US contestants.
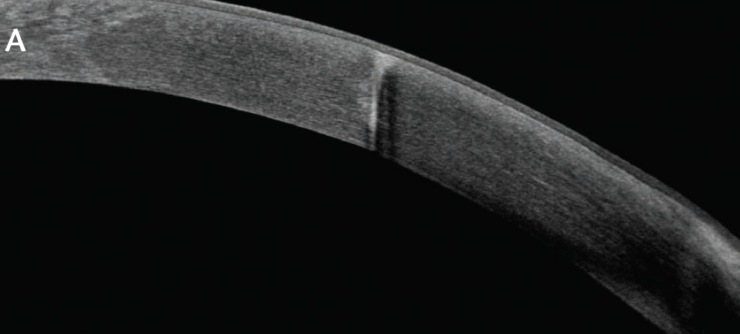
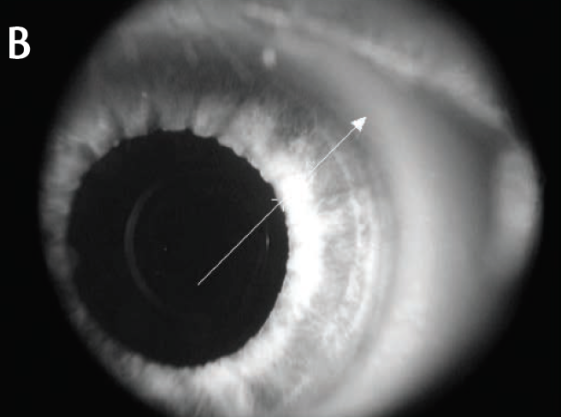
Figure 1. Inadvertent femtosecond AK within 2.5 mm of the corneal center, seen on anterior segment OCT (A) and in a slit-lamp photo (B).
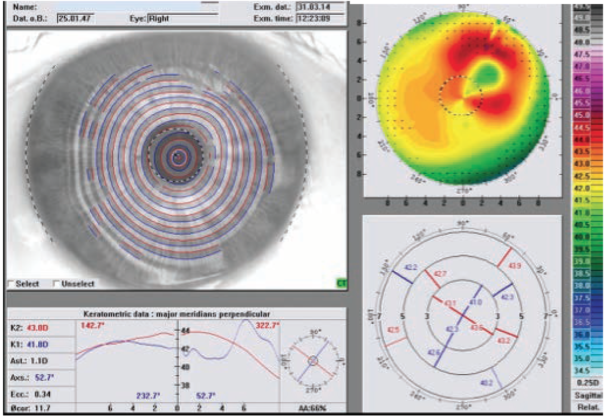
Figure 2. Topography showing significant astigmatism.
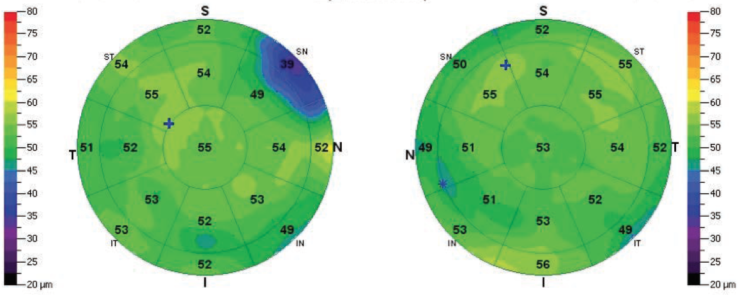
Figure 3. The blue areas on the epithelial maps correspond to the limbal AK incision.

Contestant No. 1
I presented a case exactly like this at the American-European Congress of Ophthalmic Surgery (AECOS) meeting in Aspen, Colorado, 4 years ago. The patient also had a Restor lens and was absolutely miserable. At that time in the United States, the only thing that I could do for my patient was to take the multifocal IOL out. Given the tools we have available today in the United States, I think I would still exchange the lens for a monofocal IOL.
Unfortunately, with a deep arcuate incision protruding into the 4-mm optical zone, the outlook for the long-term biomechanical stability of this cornea is poor, in my opinion. Even if you get this patient a good result that works with the multifocal IOL now, there is going to be a problem 1, 2, or even 5 years from now, John.
To your second question, for postoperative astigmatic error in a multifocal IOL patient, I would opt for wavefront-guided LASIK. To your third question, yes, I would opt for one of the presbyopia-correcting IOLs, and the amount of preoperative corneal astigmatism would dictate the IOL chosen.

Contestant No. 2
I would start by trying a rigid gas permeable (RGP) contact lens, John. If a hard contact is placed on the patient’s eye and he says, “Oh, this vision is awesome,” that might mean he can tolerate the Restor.
Another approach I would consider if I was practicing outside the United States is to assess the visual potential with a pinhole vision test. A pinhole IOL (IC-8; AcuFocus), available in some international markets, might be a way to solve this patient’s issues with presbyopia and the irregular cornea. However, I must admit that I have no personal experience with this lens or its capabilities.
Like Contestant No. 1, I would also choose LASIK as the secondary intervention for a patient with residual astigmatism after multifocal IOL implantation. If I had seen this patient initially for his cataract surgery, it would have been my choice to implant a toric presbyopia-correcting IOL.

Contestant No. 3
Before I did anything, I would want to look at this patient’s macula and optic nerve and assess his visual potential with the Potential Acuity Meter (PAM; Haag-Streit). This would help me to figure out what his best retinal vision is going to be, which is important, because, if I try something and he still ends up 20/50, I have not solved anything.
At this point, I should say that I think AKs are the third-best option for treating astigmatism at the time of cataract surgery, after (1) a toric IOL and (2) an astigmatic laser ablation. Some people still think AK has a role, but I think it is passé with the availability of better options. These incisions may look good at 3 months, but follow patients who have undergone AKs for 5, 10, or 15 years and you will see that these incisions are not astigmatically stable.
Suturing the AK is a possibility, but I did this in a patient who had AKs associated with RK, and I was not successful with it. My experience was exactly what is seen in your patient’s eye in Figure 2, the crab-claw appearance. I left the sutures in for 6 to 12 months, which may have changed the refraction in the short term, but it did not fix the problem. After 7 or 8 years, that significant crab-claw still remains. Also, in the case you presented, John, the incision is very close to the visual axis, and the suture would be even closer.
I agree with Contestant No. 1 regarding the location of the incision. It is so central that it is bound to keep on giving. A topography-guided Contoura Vision treatment (Alcon) might look good in the short term, improving the patient’s CDVA to about 20/30. But what will happen 2 or 3 years from now?
My approach to this patient would probably be lens exchange for a monofocal IOL. The combination of the multifocal IOL and the AK is causing the loss of UDVA, and eliminating the multifocal lens may gain a couple of lines of visual acuity.
To your second question, for a patient with residual astigmatism after premium IOL implantation, it would depend whether the error was hyperopic or myopic. For myopic astigmatism, my choice would be wavefront-guided LASIK. For hyperopic astigmatism, I would implant a toric piggyback IOL in the sulcus. Now, if this had been my patient from the beginning, at the time of cataract surgery, I would have chosen a toric presbyopia-correcting IOL.

Contestant No. 4
John, when I look at the patient’s topography (Figure 2) with the WaveLight Topolyzer (Alcon), the first thing I notice is that the keratometric data at the two major meridians is perpendicular (d = 3 mm). When I see so many bumps and peaks, as is the case here, then I know this is really bad. Obviously there is quite severe irregular astigmatism in the large Placido-disc corneal image; however, when I look at the small central circle representing the pupil, I notice that the astigmatism is fairly regular. That makes me think an IOL exchange might not be necessary. At this point, the patient would benefit from topography-guided Contoura LASIK given the fairly regular astigmatism on the visual axis.
If this patient was a good candidate for a toric presbyopia-correcting IOL, I would have chosen that option for the primary cataract surgery.
The Resolution
Before I talk about how this patient’s case was resolved, a few comments about our contestants’ responses, many of which were cogent and insightful. Contestant No. 2 alluded to the fact that, as anterior segment surgeons, we should always think about trying a RGP contact lens to help distinguish whether we can fix a problem on the cornea or we need to go inside to the lens.
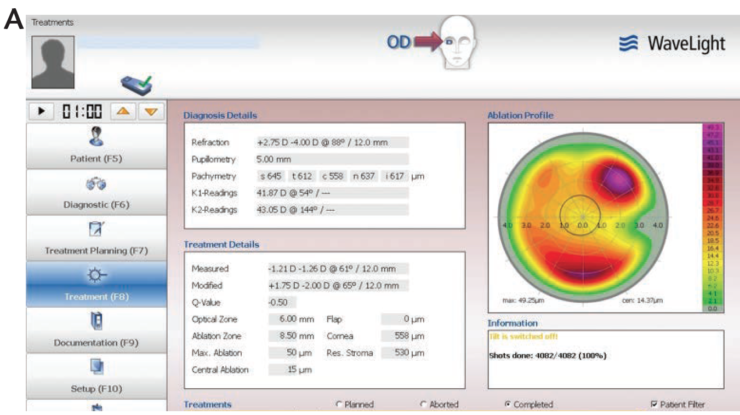
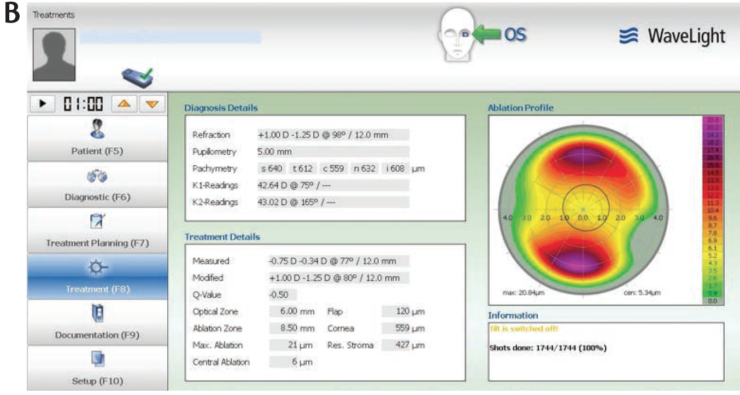
Figure 4. Topography maps of the patient’s right (A) and left (B) eyes.
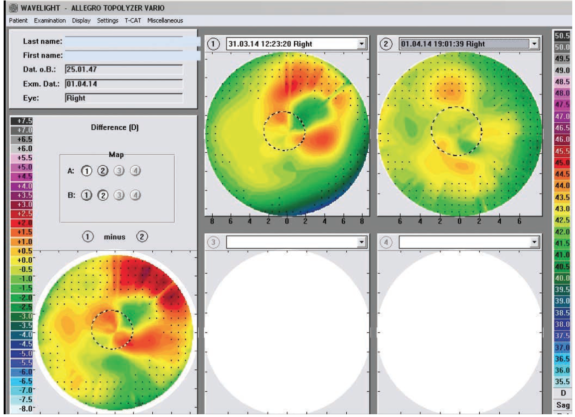
Figure 5. Pre- and postoperative topography and the ablation pattern in the patient’s right eye.
Contestant No. 3 reminded us that we need to assess retinal function so that we know whether we can solve the problem or we need to consult with a retina specialist. In our patient’s case, the retina was perfect, there was no epiretinal membrane or other problem, and the PAM result was 20/20.
Solutions proposed by the contestants centered on lens exchange. No one proposed CXL, which is not unexpected as CXL is a relatively new entity in the United States. As it happens, even though I am often an advocate for CXL, my experience in RK patients is that the treatment tends to expand the incision. So, in this cornea, CXL would probably exaggerate the refractive effect of the AK rather than reducing it. Additionally, it would stabilize the refractive effect of the AK, rather than helping to eliminate it.
I agree with Contestant No. 3 about the instability of AK. In general, I think in Europe we are not over-enthusiastic about AK, and we would opt for PRK or LASIK for residual astigmatic refractive error.
It is also notable that we had unanimous agreement that a presbyopia-correcting toric IOL would have been a good choice as a primary intervention for this patient.
In the end, after detecting residual astigmatism in the other eye, we treated both eyes with topography-guided Contoura LASIK. As you can see in Figure 4, the patient’s left eye—his better eye—had only slightly irregular astigmatism. However, the angle kappa in that eye was quite high. This speaks to a point I have been emphasizing recently: We have to rethink what regular astigmatism is. Regular astigmatism is not what is regular on the cornea, it is what is regular on the visual axis of the eye. Placido-disc topography is imaged on the corneal apex, not on the visual axis. If an eye has a large angle kappa, that regular astigmatism seen on topography is actually irregular astigmatism on the visual axis. The result in the left eye was 20/20 UDVA.
Figure 5 shows the right eye topography before and after Contoura topography-guided LASIK with femtosecond flap creation. You can see how irregular the cornea is preoperatively, and how irregular the ablation was. We got lucky, and the result was phenomenal: 20/15 UDVA.
AND THE WINNER IS...
I am impressed with all of the contestants’ responses, which essentially covered all the available anterior segment evaluation and treatment options. It is hard to pick a winner, as the contestants all approached this problem in similar fashion. I tend to like the point of view of Contestant No. 2 a little more, as I did not try a RGP contact lens and agree that, in this case, it would have been a great diagnostic tool.
GET TO KNOW THE CONTESTANTS

Contestant No. 1
Steven J. Dell, MD
• Director of Refractive and Corneal Surgery, Dell Laser Consultants, Austin, Texas
• +1 512 347-0255
• Member, CRST Europe Global Advisory Board
• Financial disclosure: Consultant (Bausch + Lomb, Abbott)

WINNER
Contestant No. 2
William F. Wiley, MD
• Private practice, Cleveland Eye Clinic, Ohio
• drwiley@clevelandeyeclinic.com
• Financial disclosure: None acknowledged

Contestant No. 3
John F. Doane, MD
• Private practice, Discover Vision Centers, Kansas and Missouri
• Clinical Assistant Professor, Department of Ophthalmology, Kansas University Medical Center, Kansas City, Kansas
• Member, CRST Europe Global Advisory Board
• jdoane@discovervision.com
• Financial disclosure: None acknowledged

Contestant No. 4
Karolinne M. Rocha, MD, PhD
• Director of Cornea Service and Assistant Professor, Storm Eye Institute, Medical University of South Carolina
• karolinnemaia@gmail.com
• Financial disclosure: Consultant (Abbott)