


Multifocal IOLs that include a third focal point for intermediate distance have become a gold standard in modern cataract surgery, providing excellent visual performance for near and intermediate vision without sacrificing distance vision.
I started implanting the Alsafit Trifocal VF lens (Alsanza) mid-year in 2016, and my preliminary clinical results to date—which include monocular and binocular visual acuity measurements for distance, near (33 cm), and intermediate (66 cm); postoperative refraction; contrast sensitivity; and assessment of photic phenomena—have been excellent. Visual acuity was tested on the Early Treatment Diabetic Retinopathy Study chart, and 90% of patients achieved monocular UDVA of 0.0 logMAR for all distances.
AT A GLANCE
• The ideal candidate for the Alsafit Trifocal VF IOL is a motivated patient with the potential for good neural adaptation, with no significant macular or optic disc changes, and with a healthy cornea with minimal corneal astigmatism.
• The sophisticated four-fin design at the end of the plate haptics facilitates self-adaptation of the IOL to different sizes of capsular bag, thereby preventing capsular retraction and maintaining effective lens position.
As expected, reading tests with binocular near and intermediate vision showed much better results compared with monocular test values. Postoperative refraction was within an acceptable range of 0.50 to -0.50 D.
The single-use Alsajet Injector system (Alsanza) allowed safe and easy implantation of the IOL through a 1.8-mm incision. As a result, no significant changes in keratometry and corneal cylinder readings were seen. These results are congruent with the fact that the lens was implanted through a very small incision.
The design of the lens provides postoperative stability with minimal induced ocular aberrations. Contrast sensitivity values were within physiologic levels. Visual phenomena were minimal; no patient complained of photic phenomena spontaneously.
CLINICAL ADVANTAGES
Currently, I prefer the Alsafit Trifocal VF IOL for several key reasons.
Reason No. 1: Patients want spectacle independence. In my experience, many patients now routinely using tablets or computers are demanding total spectacle independence for near and especially for intermediate distance. The Alsafit Trifocal VF, with adds of 1.50 D for intermediate and 3.00 D for near vision, enhances patient satisfaction for these distances without any limitation of distance vision.
Reason No. 2: The IOL corrects for spherical aberration, improving image quality postoperatively. The asphericity of the lens is -0.165 µm, correcting the spherical aberration of the typical cornea. This results in very good compensation between corneal and internal spherical aberrations, leading to low values of total ocular aberrations and improving image quality and visual performance.
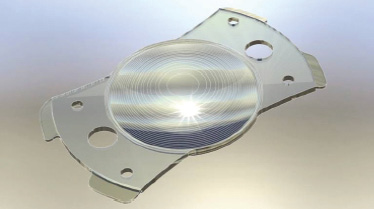
Reason No. 3: The haptic design promotes long-term stability. The combination of the great shape memory of the material and the four fins at the ends of the haptics (Figure 1) enables long-term stability and centration of the IOL in the capsular bag. The four fins, only 0.5 mm in size and located at the extremities of the haptics, allow the lens to achieve real stability in any sized bag. At the same time, the fins are made with a significant angulation of 30° to facilitate this mechanical phenomenon. To date, we have not observed any tilt or shift with this lens, inducing, for example, astigmatism in the event of capsular shrinkage. The fins play a role as pressure-absorbers and position the lens as a multifocal IOL should be positioned.
Reason No. 4: Handling and implantation of the lens is easy and safe. The one-piece, plate-haptic lens is easily implanted through a sub–2-mm incision. The 360° square edge, along with the four flexible adjustable haptic fins, creates an excellent barrier against formation of posterior capsular opacification. The four positioning holes in the haptics facilitate correct lens positioning, and the two larger holes facilitate OVD aspiration from the capsular bag (Figure 1).
The Lens: Alsafit Trifocal VF
ALSANZA
Courtesy of Alsanza
• Hydrophilic acrylic material with hydrophobic surface: glistening-free, designed to minimize posterior capsular opacification
• Provides UV and violet light filtering without compromising circadian rhythms
• Plate-haptic design with 360° square edge
• Innovative 30° angled fins at the ends of the haptics aid stability and centration
• Alsajet Injector (Alsanza) facilitates implantation through 1.8-mm incision
• Available powers: 0.00 to 32.00 D in 0.50 D steps, with 32.50 to 45.00 D available by special order
For more information: http://www.alsanza.com/alsafit-trifocal-vf/
CASE EXAMPLE
The Alsafit Trifocal is appropriate for many patients who wish to achieve spectacle independence postoperatively. Sometimes, as with the case example below, it can be especially valuable.
A 45-year-old emmetrope requested lens surgery with multifocal IOL implantation. He works as a car mechanic and is frequently under scotopic and mesopic light conditions. Preoperatively, his UDVA was 0.0 logMAR, UIVA was 0.3 logMAR, and UNVA was 0.4 logMAR. Although interested in lens exchange surgery, he was concerned about the potential for worsening of contrast sensitivity and the occurrence of visual phenomena. His most important demand was improvement of vision at a working distance of about 60 to 70 cm.
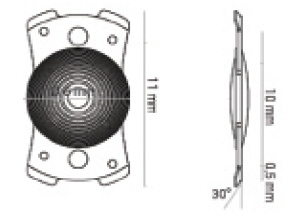
Figure 1. Specifications of the Alsafit Trifocal VF.
The goal for this patient was to maintain distance vision and focus on improving vision at working distance. I decided to implant the Alsafit Trifocal VF because of its low addition for intermediate vision. Surgery was performed without any complications; the lens was implanted through a 1.8-mm incision in the capsular bag. OVD was completely removed using the two large holes in the lens haptics.
Postoperatively, the patient was extremely happy. He achieved 0.0 logMAR at all distances, without visual phenomena.
POINTERS AND PEARLS
Clinical use of this lens is much the same as for any other multifocal or trifocal IOL. Every patient should undergo a comprehensive preoperative ocular examination. In planning surgery, patient selection is crucial.
The ideal patient is a motivated hyperope with the potential for good neural adaptation, with no significant macular or optic disc changes, and with a healthy cornea with minimal corneal astigmatism. In eyes with higher degrees of corneal astigmatism, the Alsafit Trifocal Toric VF lens is indicated.
Challenging cases include emmetropes and low myopes because of the potential for dissatisfaction even after successful surgery. At present, I recommend this lens with its low near and intermediate adds because most of my patients use computers in their jobs or desire perfect working vision at a distance of arm’s length.
There are two notable points to remember about this trifocal lens. First, the sophisticated four-fin design at the end of the plate haptics facilitates self-adaptation of the IOL to different sizes of capsular bag, thereby preventing capsular retraction and maintaining effective lens position. Second, this lens is manufactured in a huge dioptric range, from 0.00 to 32.00 D, with up to 45.00 D available by special order.
