


The SBL-3 IOL (Lenstec) is designed to provide excellent distance, intermediate, and near vision; improve contrast sensitivity; and reduce dysphotopsias. A clinical study found excellent objective and subjective outcomes 3 months postoperatively, with 94.4% of patients reporting they were very satisfied or satisfied.1
AT A GLANCE
• The SBL-3 IOL displays high tolerance in myopic, hyperopic, and emmetropic patients, especially with a lower add in the dominant eye.
• The SBL-3 is suitable for presbyopic patients and for prepresbyopic patients with refractive errors not suitable for laser corneal surgery or phakic IOL implantation; preoperative pupil assessment is essential.
To date, one of us (JEM) has implanted approximately 250 of these IOLs with excellent outcomes. In a study submitted for publication, we documented the outcomes of the SBL-3 IOL at 3 and 12 months postoperatively. Patients were asked to rate their quality of vision (QOV) on a scale of 0 (worst) to 10 (best). At the initial postoperative assessment, the mean QOV score was 8.26 ±1.16, increasing to 8.84 ±1.08 at 12 months. Additionally, 42 of 45 patients reported never needing reading glasses, and three reported requiring glasses only occasionally.
PREOPERATIVE FACTORS
Because of the nature of asymmetric multifocal IOLs, postoperative outcomes can be affected by three key factors: IOL centration, pupil diameter, and pupil shift. Each of these factors has the potential to affect the performance of the IOL because adequate exposure of the two distinct segments within the pupil diameter is required.
The Lens: SBL-3
LENSTEC
• Rotationally asymmetric multifocal IOL
• Optic size 5.75 mm, with biaspheric zero-aberration design to enhance depth of focus
• An asymmetric 3.00 D sector-shaped near add zone and an aspheric distance zone are separated by a small wedge-shaped transition zone
• Light is reflected away from the optical axis when it hits this transition zone
• Overall length 11 mm; modified plate haptics with 0° angulation
• Square posterior edge
• Sphere powers from 10.00 to 36.00 D, with the 15.00 to 25.00 D range in 0.25 D steps
• Manufactured to ±0.11 D power accuracy
• One-piece acrylic with 26% water content; can be implanted through a microincision
For more information: http://www.lenstec.com/sbl-3.html

Courtesy of Lenstec
Factor No. 1: Adequate pupil diameter. To ensure optimal performance of the SBL-3 IOL, therefore, adequate pupil diameter is required. A study by Pazo et al (submitted for publication) assessed the effect of pupil size on outcomes after SBL-3 IOL implantation. This study found that subjective QOV was significantly lower in eyes with pupil sizes less than 3 mm, even though there was no significant difference in objective visual outcomes.
This study also highlighted that patients’ photopic pupil sizes significantly decreased from preoperative assessment to final postoperative assessment. It is important to be aware that pupil diameter decreases with age, and selecting patients with adequate preoperative pupil size is essential to maintaining high patient satisfaction despite decreasing pupil diameter with age.
Pazo et al found that preoperative pupil size greater than 3 mm is adequate to maintain a high level of QOV (≥8.3). Because there is, in general, a small progressive reduction in pupil size over the following postoperative 3 years, it is prudent to consider this when defining an optimal target preoperative pupil size.2
Factor No. 2: Position of the near addition. Another key preoperative consideration when implanting the SBL-3 IOL is the position of the near addition. A case report by Pazo et al described a patient who, after SBL-3 implantation, complained of blurred vision when driving during the day and in supermarkets.3 On assessment of IOL position, it was noted that, in the patient’s dominant eye, there was high exposure of the near segment to the detriment of the distance portion. The IOL in the dominant eye was therefore rotated from an inferonasal to a superotemporal position to optimize the distance segment exposure within the mesopic and photopic pupil (Figure 1). Three months after rotation surgery, the patient showed improved visual acuity and better QOV and was pleased with vision both when driving and in the supermarket.
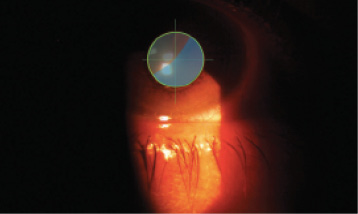
Figure 1. Pupil assessment of the right eye of a patient after rotation of the IOL. The near segment is now positioned superotemporally. Pupil assessment is performed by overlaying a retroillumination image from the slit lamp.
Based on this case report and other studies highlighting that asymmetric multifocal IOLs can be placed in other rotational positions without negatively affecting postoperative outcomes,4,5 we sought to compare superotemporal placement of the near segment in the dominant eye combined with inferonasal placement in the fellow eye (Figure 2) with bilateral inferonsal placement of near segments.6 Additionally, in the dominant eye with superotemporal placement, we implanted IOLs with a lower add (2.00 D), which have been found to provide full distance and intermediate vision rehabilitation but reduced UNVA when compared to IOLs with 3.00 D add.7,8
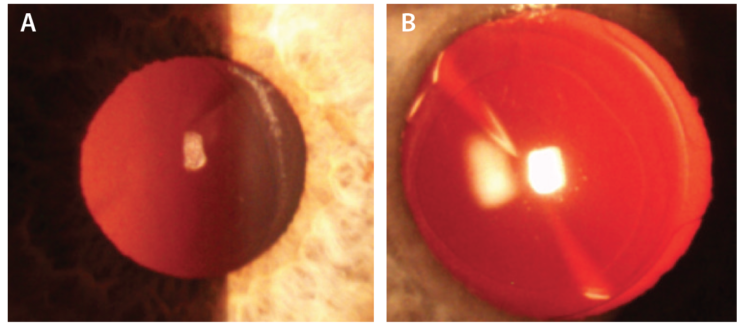
Figure 2. Retoillumination images of superotemporal placement of the near segment (2.00 D add) in the dominant eye (A) and inferonasal placement of the near segment (3.00 D add) in the nondominant eye (B).
Our results indicated that superotemporal placement of the lower-power add in the dominant eye combined with inferonasal placement of the 3.00 D near add in the nondominant eye can provide superior QOV to bilateral inferonasal 3.00 D near segment placement. Another benefit of using this IOL combination is that it improves functional intermediate vision, as 83.3% of patients reported clear vision at this distance. Bilateral inferonasal 3.00 D add placement also provided excellent UIVA,1 but we have found that a lower percentage of patients (73.3%) reported completely clear intermediate vision with this arrangement.
We recommend ensuring a preoperative photopic pupil size of greater than 3 mm, with combined superotemporal and inferonasal placement of near segments, to protect against long-term changes in pupil size and subsequent loss of vision through inadequate exposure of either the distance or near zones.
PATIENT SELECTION
The SBL-3 is suitable for presbyopic patients and for prepresbyopic patients with refractive errors not suitable for laser corneal surgery or phakic IOL implantation. Patients who have had previous hyperopic laser surgery and those with any active ocular disease should be avoided.
In patients with amblyopia, the amblyopic eye should not be fitted with an asymmetric multifocal IOL. The amblyopic eye can be fitted with a monofocal IOL (target 0.00 to -1.00 D if it is the nondominant eye) in combination with an asymmetric multifocal IOL in the nonamblyopic eye. The nonamblyopic eye must, however, have a sufficient photopic pupil diameter of greater than 3.5 mm.
We recommend the use of a capsular tension ring in all surgeries to facilitate subsequent IOL rotation or explantation. Preoperative pupil assessment is essential, and we actively assess all patients with the Aladdin biometry and topography system (Topcon). This instrument gives information on photopic and mesopic pupil diameters, pupil shift, and pupil centration, which aids the surgeon’s decision on IOL placement and near add power. Other instruments can give similar pupil information.
CONCLUSION
We like to use the SBL-3 IOL because it displays high tolerance in myopic, hyperopic, and emmetropic patients, especially with a lower add in the dominant eye. One must keep in mind that pupil diameters must be assessed and that only patients with adequate photopic pupil diameters should be selected.
1. Venter JA, Barclay D, Pelouskova M, Bull CE. Initial experience with a new refractive rotationally asymmetric multifocal intraocular lens. J Refract Surg. 2014;30(11):770-776.
2. Pazo EE. Optimal pupil size for asymmetrical multifocal intraocular lenses. Paper presented at: European Society of Cataract and Refractive Surgeons Annual Meeting; September 10-14, 2016; Copenhagen, Denmark.
3. Pazo EE, Richoz O, McNeely R, Millar ZA, Moore TC, Moore JE. Optimized visual outcome after asymmetrical multifocal IOL rotation. J Refract Surg. 2016;32(7):494-496.
4. de Wit DW, Diaz J, Moore TC, Moutari S, Moore JE. Effect of position of near addition in an asymmetric refractive multifocal intraocular lens on quality of vision. J Cataract Refract Surg. 2015;41(5):945-955.
5. Song IS, Yoon SY, Kim JY, Kim MJ, Tchah H. Influence of near-segment positioning in a rotationally asymmetric multifocal intraocular lens. J Refract Surg. 2016;32(4):238-243.
6. McNeely RN, Pazo EE, Spence A, et al. Comparison of the visual performance and quality of vision with combined symmetrical inferonasal near addition versus inferonasal and superotemporal placement of rotationally asymmetric refractive multifocal intraocular lenses. J Cataract Refract Surg [in press].
7. Alió JL, Plaza-Puche AB, Piñero DP, Javaloy J, Ayala MJ. Comparative analysis of the clinical outcomes with 2 multifocal intraocular lens models with rotational asymmetry. J Cataract Refract Surg. 2011;37:1605-1614.
8. Alió JL, Plaza-Puche AB, Montalban R, Javaloy J. Visual outcomes with a single-optic accommodating intraocular lens and a low-addition-power rotational asymmetric multifocal intraocular lens. J Cataract Refract Surg. 2012;38:978-985.

