



Since its introduction, laser-assisted cataract surgery (LACS) has become a well-established technique with a robust literature supporting its efficacy and safety, including many papers to which I have contributed.1-4 I was the first surgeon in Spain to perform LACS with the LenSx Laser (Alcon).
AT A GLANCE
• Femtosecond laser technology has brought added precision to several steps of cataract surgery that previously demanded high levels of surgeon skill.
• According to results of one computer-based economic modeling study, to make LACS cost-effective to the patient, reduced per-click fees and costs of consumables would be needed.
• In one estimation, current consumables and click fees for LACS amount to more than €300 per eye.
Nonetheless, despite my extensive positive experience with the clinical results of this innovative advanced-technology surgery, I no longer perform LACS. This is not because of technical aspects of the surgery, but rather because I believe the cost is unsustainable in the current economic climate. This article outlines some of my experience with LACS and that of other surgeons, as reflected in the published literature, and ends with my rationale for setting the technique aside—at least for the time being.
REVOLUTIONARY TECHNOLOGY
Femtosecond laser technology has brought added precision to several steps of cataract surgery that previously demanded high levels of surgeon skill. The ability of the laser systems to form a perfectly round capsulotomy is perhaps most greatly appreciated by cataract surgeons, but the incision creation and lens fragmentation capabilities are also highly valued. These functions help to decrease surgical time and reduce or even eliminate the need for phacoemulsification energy for cataract removal.1
My experience with this technology began with the LenSx Laser, the first laser used clinically in Europe for LACS. It was also the first ophthalmic femtosecond laser to receive clearance by the US FDA, in 2009, and it currently has three FDA indications, for anterior capsulotomy, corneal incision creation, and lens fragmentation. It received the CE Mark in 2011.
RESULTS OF A PROSPECTIVE CASE SERIES
In this interventional prospective case series, 94 eyes were randomly assigned to one of four groups: microincision LACS with a 1.8-mm incision, microcoaxial LACS with a 2.2-mm incision, microincision phacoemulsification with a 1.8-mm incision, or microcoaxial phacoemulsification with a 2.2-mm incision. In the phacoemulsification arms, continuous curvilinear capsulorrhexis was performed. To avoid the influence of a learning curve, the three surgeons in the study each excluded their first 10 LACS cases. Only grade 3 cataracts were included, and mean age was similar in the four groups. Outcomes at 1-month follow-up were analyzed.
We found that all laser-created corneal incisions were easy to open with a blunt spatula, and all were self-sealing. Dimensional reproducibility was excellent, with standard deviation of ±0.1 mm for incision width and ±5.2° for incision angle.
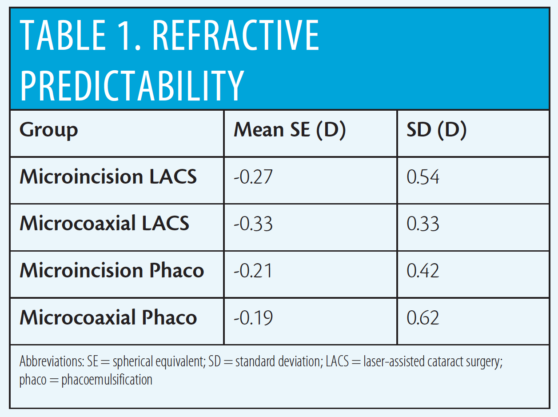
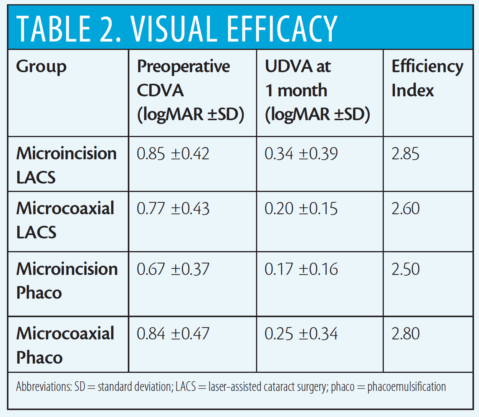
Refractive predictability (Table 1) and visual acuity results (Table 2) were similar among the four groups. In terms of visual efficacy, preoperative CDVA was similar among all groups (P>0.5 for all comparisons) and postoperative UDVA was similar among all groups (P>0.5 for all comparisons) using analysis of variance. Efficiency index ranged from 2.50 to 2.85 among the groups.
Safety outcomes were excellent in the study. No significant changes in pachymetry, endothelial cell count, or macular thickness were seen from preoperative to 1 month postoperative in eyes undergoing LACS procedures. Surgical incidents during LACS procedures included suction loss in three eyes (4.4%), no cone recognition in three eyes (4.4%), and petechiae in 50% of eyes of patients older than 70 years. Surgical incidents during phacoemulsification in the LACS eyes included one (2.1%) posterior capsular rupture, two (4.2%) anterior capsular tears with no posterior extension, and two (4.2%) capsular bridges that were corrected with forceps. After phacoemulsification, there was leakage from incisions in six cases.
Like many other surgeons, I used the laser for those three functions: corneal incisions, capsulotomy, and photodisruption of the nucleus. The incorporated OCT facilitated treatment planning and allowed us to see the laser in action as it performed our chosen parameters.
Colleagues and I performed a study to assess the efficacy and safety of cataract surgery assisted by femtosecond laser technology in comparison with conventional phacoemulsification (see Results of a Prospective Case Series).2,3 To summarize these results and my own clinical impressions, compared with standard phacoemulsification techniques, with LACS there was a large improvement in control of the quality of the capsulotomy and a real improvement in the lens aspiration and emulsification process (although with a decrease in mean ultrasound power only in the microincision LACS group) and a reduction in the time of the total intraocular procedure. There was not, however, an improvement in the quality of corneal incisions. After analyzing our results, I have the impression that LACS is a better, more advanced version of cataract surgery than traditional phacoemulsification.
Yet I wonder whether this advance comes at an affordable cost.
ECONOMIC IMPACT
Although the promise of LACS was apparent to me and to other investigators from the moment of its introduction, so was the problem of its practicality. When I reviewed the emerging technologies for LACS in 2011, I predicted that “a new path for the future of cataract surgery” was opening, but, in the same publication, I raised the issue of the increased costs associated with incorporating this expensive laser technology into practice.1
Others have also expressed concerns about the cost-effectiveness of LACS. Abell and Vote attracted much attention in 2014 when their computer-based economic modeling study concluded that LACS is not cost-effective.5 They performed a cost-effectiveness analysis comparing conventional phacoemulsification with LACS in a hypothetical cohort of patients undergoing cataract surgery. Improvements in CDVA based on current literature were used to calculate the quality-adjusted life-years in their hypothetical cohort, and this was combined with approximate costs in a cost-utility analysis model.
These authors concluded that, irrespective of potential improvements in visual acuity outcomes and reduction of complication rates, LACS is not cost-effective at its current cost to the patient, when considered against cost-effectiveness benchmarks. A considerable reduction in cost to the patient—possibly through reduced per-click fees and costs of consumables—would be needed for LACS to be considered cost-effective, they stated.
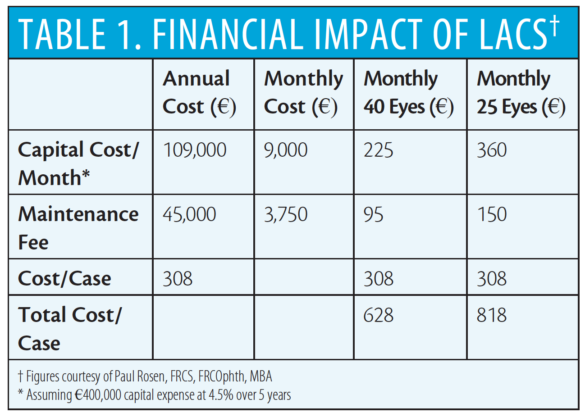
Paul Rosen, FRCS, FRCOphth, MBA, has estimated some of the costs added to cataract surgery when LACS is performed. The capital cost of the laser he estimates at €400,000, with financing costs at 4.5% and a maintenance fee of €45,000 per year. Consumables and click fees amount to more than €300 per eye. These costs would be further augmented by extra chair time to explain the procedure to patients, additional staff, the increased operating room time to implement the new technology, and marketing costs specific to the practice’s use of the femtosecond laser. His estimations of total costs based on these figures are shown in Table 1 on the following page.
CONCLUSION
I have set aside LACS, at least at its current cost. Clearly the technology brings precision to certain surgical steps and helps to reduce or eliminate the need for phacoemulsification energy inside the eye. However, the benefits of the procedure in terms of improvement in visual acuity outcomes are incremental at best. In our study comparing conventional phacoemulsification and LACS, visual acuity results were similar in all groups.
Given the significant costs associated with use of the technology, LACS presents a difficult financial model for today’s cataract surgical practice, at least in the economic environment of the European Union. I do not find LACS, with its current capital and per-eye costs, to be a cost-effective procedure for my patients, whether in the private or the public health care system. If costs can be reduced, or if the economic climate changes in some other way, perhaps in the future I can consider readopting this technology for my cataract patients.
1. Alió JL. Cataract surgery with femtosecond lasers. Saudi J Ophthalmol. 2011;25(3):219-223.
2. Miháltz K, Knorz MC, Alió JL, et al. Internal aberrations and optical quality after femtosecond laser anterior capsulotomy in cataract surgery. J Refract Surg. 2011;27(10):711-716.
3. Nagy ZZ, Filkorn T, Takács AI, et al. Anterior segment OCT imaging after femtosecond laser cataract surgery. J Refract Surg. 2013;29(2):110-112.
4. Roberts TV, Lawless M, Bali SJ, Hodge C, Sutton G. Surgical outcomes and safety of femtosecond laser cataract surgery: a prospective study of 1500 consecutive cases. Ophthalmology. 2013;120(2):227-233.
5. Abell RG, Vote BJ. Cost-effectiveness of femtosecond laser-assisted cataract surgery versus phacoemulsification cataract surgery. Ophthalmology. 2014;121(1):10-16.
Additional reading:
1. Ashok G, Alió JL. Femtosecond laser techniques and technology. Jaypee Brothers Medical Publishers; 2012.
2. Alió JL, Abdou AA, Puente AA, Zato MA, Nagy Z. Femtosecond laser cataract surgery: updates on technologies and outcomes. J Refract Surg. 2014;30(6):420-427.
3. Alió JL, Soria F, Abdou AA, Peña-García P, Fernández-Buenaga R, Javaloy J. Comparative outcomes of bimanual MICS and 2.2-mm coaxial phacoemulsification assisted by femtosecond technology. J Refract Surg. 2014;30(1):34-40.
4. Alio JL, Soria F, Abdou AA. Femtosecond laser assisted cataract surgery followed by coaxial phacoemulsification or microincisional cataract surgery: differences and advantages. Curr Opin Ophthalmol. 2014;25(1):81-88.
5. Alió JL, Abdou AA, Soria F, Javaloy J, Fernández-Buenaga R, Nagy ZZ, Filkorn T. Femtosecond laser cataract incision morphology and corneal higher-order aberration analysis. J Refract Surg. 2013;29(9):590-595.
6. Popovic M, Campos-Möller X, Schlenker MB, Ahmed II. Efficacy and safety of femtosecond laser-assisted cataract surgery compared with manual cataract surgery: a meta-analysis of 14 567 eyes. Ophthalmology. 2016;123(10):2113-2126.