


REFRACTIVE SURGERY
It Takes Two To Tango: Collaborative Care Approach to Refractive Surgery
By Cecelia Koetting, OD, FAAO
From 2006 to 2016, the number of ophthalmic resident positions in the United States grew only slightly, from 447 to 469,1 and the number of practicing opthalmologists who are retiring continues to rise. One strategy to combat the shortage of ophthalmologists, Dr. Koetting says, is collaborative care. Shared patient care can be accomplished by developing relationships and good rapports with optometrists. One way to begin to build those relationships is by reaching out to local providers to see who is receptive to this type of patient care, Dr. Koetting advises.
TRAILBLAZERS
Simplifying the Preoperative Evaluation Process
By Andrew S. Morgenstern, OD, FAAO; and William B. Trattler, MD
Data gathered during the preoperative examination in patients scheduled for CXL is extremely important because these baseline measurements are used as a point of comparison for every future examination, Drs. Morgenstern and Trattler explain. The accuracy of these readings, which typically include refraction, UCVA, BCVA, topography, tomography, IOP, and corneal thickness, should be maximized. The best way to do so, the physicians say, is by using modern technology such as Scheimpflug photography and OCT.
Managing Progression After CXL
By Kathryn M. Hatch, MD
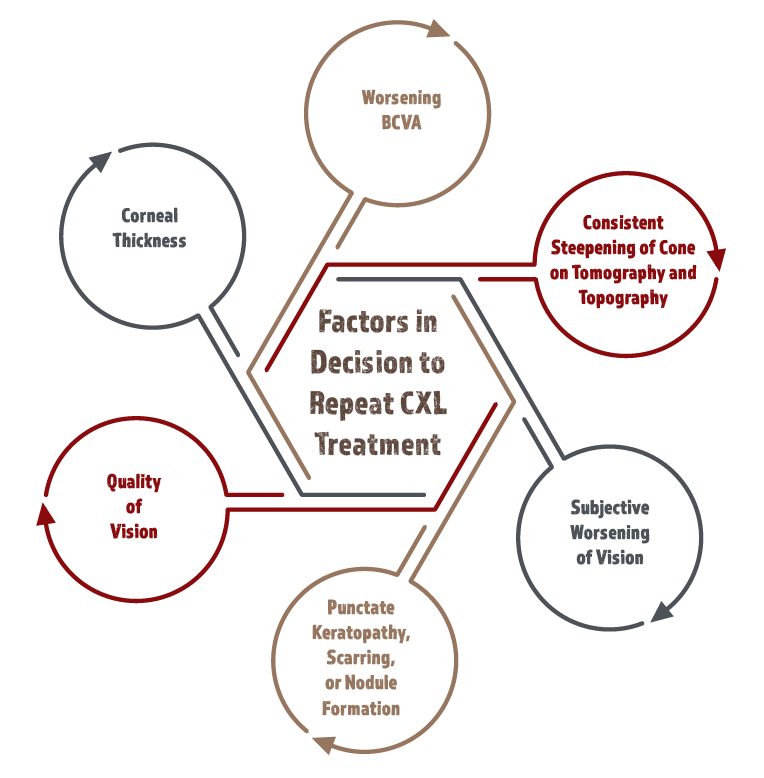
A major challenge in managing keratoconus progression is identifying it, Dr. Hatch cautions. Common marks of disease progression after CXL are an increase of more than 0.50 to 1.00 D in maximum keratometry, extreme corneal thinning (<330 µm), and more eccentrically located cones. Ensure that the cornea is 400 µm or thicker prior to CXL treatment to prevent endothelial damage and to improve the efficacy of treatment, Dr. Hatch advises. But when signs of progression are clear, including corneal thickness, worsening BCVA and subjective worsening of vision, consistent steepening of the cone, punctate keratopathy, scarring, and nodule formation, consider CXL retreatment.
1. Ophthalmology Residency. SF Match Residency and Fellowship Matching Services. https://www.sfmatch.org/SpecialtyInsideAll.aspx?id=6&typ=2&name=Ophthalmology#. Accessed August 22, 2017.


