



Those of us who use the internet (in other words, all of us) have noticed that the recommendations, questions, and advertisements automatically directed to us online have become highly personalized. This is because companies follow our activities closely by monitoring our use of the internet and social media networks. Tracking activities in this way allows companies to create personal behavior profiles that represent our lifestyles and expectations.
In the same way, digitalization and the use of big data are now facilitating the monitoring of patient behavior. This new trend, which already has begun to individualize our health and well-being, will ultimately benefit cataract and refractive surgeons and their patients.
SUBJECTIVE VERSUS OBJECTIVE
It is important for us to understand our patients’ individual needs, demands, and expectations for our treatments, in particular for premium refractive cataract surgery solutions. However, our current standard of care for customizing treatments is limited to the subjective method of asking patients about their behaviors, vision needs, and expectations.
Our questions and questionnaires serve two purposes. First, they help patients to understand the benefits of a premium procedure (eg, a multifocal IOL). Second, they help surgeons to understand patients, with the intention to provide the best and most affordable solution for the proposed life-changing treatment.
A questionnaire is a subjective method of self-reporting consisting of a set of questions, usually in a structured form. The main strength of self-reporting is that it allows users to describe their own experiences. It can be used to examine a large number of variables and to reveal behaviors and feelings that patients have experienced in real-life situations. The drawback, however, is that the users may not respond truthfully—sometimes because they cannot remember, sometimes because they wish to present themselves in a socially acceptable manner, and sometimes because they might have a different understanding of the questions due to language or cultural differences. Consequently, questionnaires are often said to lack validity.
What if we could use an objective visual behavior tool to customize patient care? The Visual Behavior Monitor device (VBM; Vivior) attaches to the user’s spectacles, typically for 8 to 10 hours daily for 3 to 5 days. During this time, the device measures the user’s refractive needs and the direction of his or her gaze by measuring the view distances with optical sensors. Further sensors detect the motion of the subject and environmental conditions such as the levels of visible and UV light.
The device does not use cameras or microphones and thus cannot compromise the privacy of the wearers or those around them. Data are sampled several times per second, generating a large data set of distances, head and body motions, and light conditions. This big data set is uploaded to a server in the cloud and processed via artificial intelligence to derive a picture of the activities and behaviors of the individual (Figure 1). It can then be visualized via a web interface for patient education by the health care provider. Further, surgeons can access the system to evaluate the patient’s suitability for a multifocal IOL and to select the best possible lens based on that individual’s vision needs.
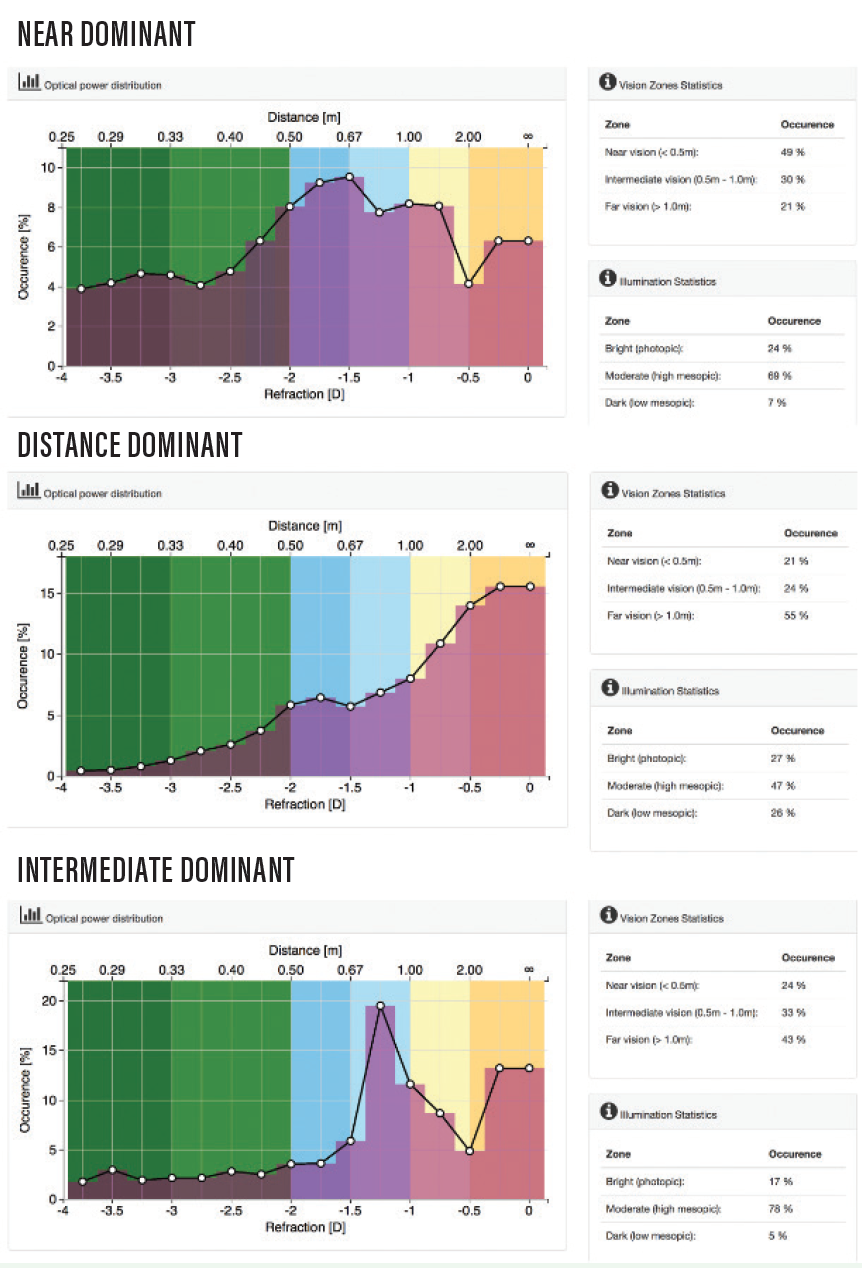
Figure 1. Examples of VBM readouts from three patients.
CLINICAL STUDY
In a prospective clinical study at Medipol University, the VBM was used to assess the differences among 48 patients’ distance, intermediate, and near vision needs. The data from the study were processed, and mean percentages of the most time spent at each distance were determined. Only one-third of patients had distance dominance (45% or more of the time used for distance vision). This indicated that the participants involved in the study used much less distance vision than was evaluated by the physician, who was masked to the VBM measurement results.
The findings indicated that patients’ near and intermediate dominance needs may be higher than we assumed. As a possible consequence, we may underestimate patients’ near vision needs, and they may be disappointed if their premium solution does not support their vision behavior needs.
Our study also demonstrated that there is a need for objective, reproducible scientific data to assist physicians in understanding and evaluating their patients’ needs. Relying on patients to remember their activities themselves, as we do with self-reporting questionnaires, risks our being misled about their needs and behaviors. Moreover, patients’ estimates may reflect unconscious biases. In one study using a near-work analyzer, subjective, self-reported estimates of working distances correlated poorly with objective measurements.1 That study showed that individuals with closer working distances tended to overestimate their reading distances, but those with farther working distances tended to underestimate them. The investigators suggested that this might have been due to a bias among patients toward a perceived normal average value.
DISCERNING PATIENTS’ NEEDS
Multifocal IOLs are designed to provide clear vision at more than one focal point, but patients still need to prioritize their visual needs in order to help us choose the appropriate IOL. This requires that the surgeon understand each patient’s lifestyle: How many hours each day does he or she spend driving, walking, reading, at the computer, playing a musical instrument, playing golf or tennis? Only when the surgeon understands the patient’s activities well enough to make an accurate judgment about his or her distance needs can a lens be chosen that will best meet that patient’s vision requirements.
OTHER APPLICATIONS
Recently, the VBM was used to calculate an optical design for progressive spectacle lenses (also called progressive addition lenses). This design was then used to manufacture spectacle lenses, which are currently being tested. The optical corrections were calculated and produced using objective measurements of real-life visual behavior, not based on statistics or historical self-reported data. The tests being performed with these spectacles will be an initial step to demonstrate the possibilities of using objective data to customize vision correction solutions with IOLs or other surgical refractive procedures.
Another future field of application for the VBM is analysis and monitoring of progressive myopia. The prevalence of myopia has markedly increased in the past 2 decades, particularly in East Asia. Recent studies in this region have shown that 80% to 90% of 18-year-old school children are myopic and 10% to 20% of teenagers are highly myopic (-6.00 D).2 The VBM can help us to understand the lifestyles of children with progressive myopia and educate their parents accordingly.
In one study, myopic axial elongation during a 4-year period was associated with shorter time spent outdoors, longer time spent indoors studying, and parental myopia. Other factors such as level of parental education, family income, gender, and region of habitation were significantly associated with axial elongation and with myopia progression only in univariate analysis.3
In our own study,4 the VBM device helped us to better analyze the progression of myopia in children (Figure 2). In 83% of 30 children with a mean age of 11 ±2.7 years with myopic progression, close (< 50 cm) working time constituted more than 45% of total time measured. Further, 90% of the children had a mean percentage of less than 25% photopic illuminance—that is, outdoor activities and high light levels (> 50 lux)—during their daily activities.
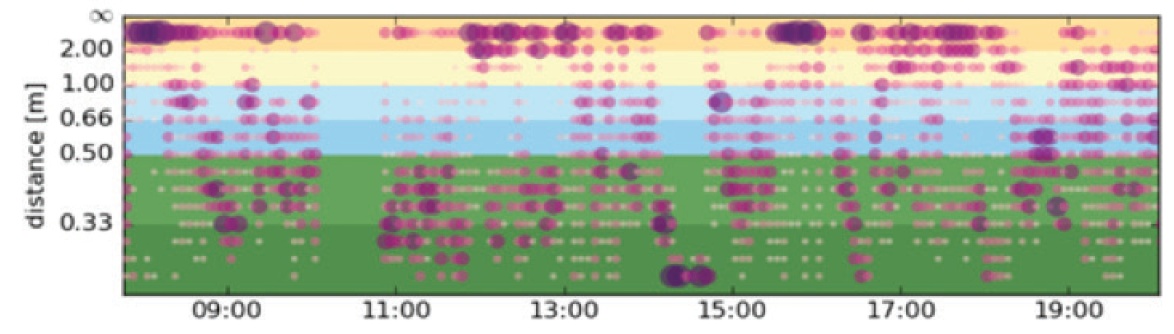
Figure 2. Daily visual distance and direction graphs for a child with progressive myopia. This child had high near vision use throughout the day, with two near peaks at approximately 40 and 25 cm.
CONCLUSION
The VBM provides useful, objective information that can help surgeons to understand the daily visual behaviors of their patients. Using data from the VBM, surgeons can customize and personalize their treatments, which ultimately will improve clinical outcomes for them and for their patients.
1. Leung TW, Flitcroft DI, Wallman J, et al. A novel instrument for logging nearwork distance. Ophthalmic Physiol Opt. 2011;31(2):137-144.
2. You QS, Wu LJ, Duan JL, et al. Prevalence of myopia in school children in greater Beijing: the Beijing childhood eye study. Acta Ophthalmol. 2014;92:e398-406.
3. Guo Y, Liu LJ, Tang P, et al. Outdoor activity and myopia progression in 4-year follow-up of Chinese primary school children: The Beijing children eye study. PLoS One. 2017;12(4):e0175921.
4. Tabakcı BN, Tanrıverdi C, Kılıç A, Mrochen M. Evaluation of daily near activities distance in progressive myopic children. Poster presented at: ARVO 2019; May 3-7, 2019; Vancouver, British Columbia.