
Refractive surgery patients have high expectations when it comes to their eyes. It is no longer enough to provide patients with great vision; we must also provide them with an experience that they will remember fondly and share with friends and family.
In our opinion, the VisuMax femtosecond laser (Carl Zeiss Meditec) is one of the key elements in creating a pleasant surgical experience. The primary reason is the lack of any sensation while the eye is immobilized under suction (Figure). The VisuMax uses a curved contact glass that requires very low suction to stabilize the eye during treatment. The low vacuum of the VisuMax eliminates the total blackout phase of surgery, as blood can continue to flow through the eye during the entire procedure. Additionally, the system limits distortion of the corneal lamellae, thus enabling optically smooth cuts and, hence, SMILE. Both of us can speak to this from first-hand experience: We both had LASIK, performing the surgery for each other.
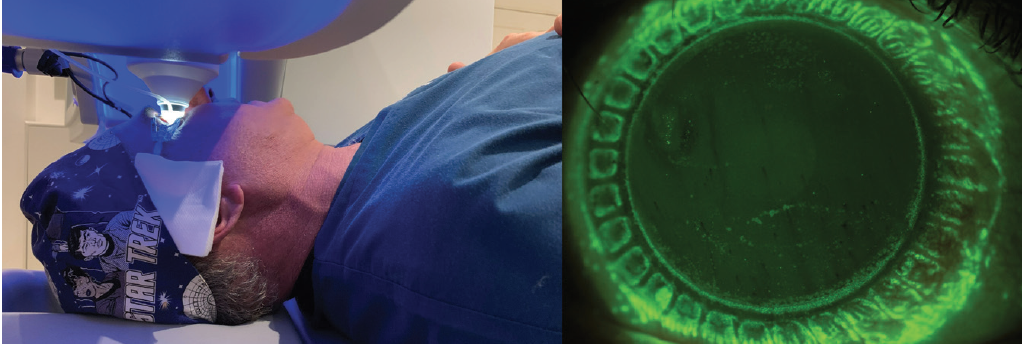
Figure. Dr. Reinstein under the VisuMax during suction (left) and immediately after under fluorescein staining (right) to demonstrate peripheral attachment of the suction ports on the corneolimbal periphery.
The average time to make a LASIK flap with the VisuMax is 20 seconds, which includes the docking phase. This short duration creates a wow factor for patients. Because the VisuMax uses very small laser spots combined with very low energy, there is little to no opaque bubble layer coalescence. This allows us to set infrared-based eye tracking on the MEL 90 (Carl Zeiss Meditec) immediately after flap creation and enables most patients to see well immediately after surgery. The low energy required to create tissue separation also decreases the chance of patients experiencing transient light sensitivity or inflammation in the early postoperative period.
The VisuMax is currently the only femtosecond laser that is approved to perform SMILE. One of the biggest advantages from a patient experience standpoint is the marked reduction in amount and duration of postoperative impaired corneal sensitivity and dry eye compared with LASIK.1 Just as with LASIK, most patients see very well the day after treatment. In our clinic, more than 80% of myopic patients are treated using SMILE.
Conclusion
The VisuMax is the workhorse of our clinic. Its unique characteristics and its accuracy and reproducibility (to within 4.4 µm)2 make it the ideal device for creating flaps in LASIK and lenticules in SMILE. The reproducible flap thickness enables the safe use of ultra-thin (80 µm) flaps,3 and it provides the option for retreatment after SMILE by thin-flap LASIK,4 Circle,5 or sidecut only.4
In addition to these refractive surgery treatments, the VisuMax can be used in other applications such as penetrating keratoplasty,6 deep anterior lamellar keratoplasty,7 and intrastromal corneal ring channel implantation.8 We and others are exploring further applications such as donor lenticule implantation9 and sutureless corneal transplantation.10
1. Reinstein DZ, Archer TJ, Gobbe M, Bartoli E. Corneal sensitivity after small-incision lenticule extraction and laser in situ keratomileusis. J Cataract Refract Surg. 2015;41:1580-1587.
2. Reinstein DZ, Archer TJ, Gobbe M. Accuracy and reproducibility of cap thickness in small incision lenticule extraction. J Refract Surg. 2013;29:810-815.
3. Reinstein DZ, Carp GI, Archer TJ, et al. Long-term visual and refractive outcomes after LASIK for high myopia and astigmatism from -8.00 to -14.25 D. J Refract Surg. 2016;32:290-297.
4. Reinstein DZ, Carp GI, Archer TJ, Vida RS. Inferior pseudo-hinge fulcrum technique and intraoperative complications of laser in situ keratomileusis retreatment after small-incision lenticule extraction. J Cataract Refract Surg. 2018;44:1355-1362.
5. Siedlecki J, Luft N, Mayer WJ, et al. CIRCLE enhancement after myopic SMILE. J Refract Surg. 2018;34:304-309.
6. Kamiya K, Kobashi H, Shimizu K, Igarashi A. Clinical outcomes of penetrating keratoplasty performed with the VisuMax femtosecond laser system and comparison with conventional penetrating keratoplasty. PLoS One. 2014;9:e105464.
7. Lu Y, Chen X, Yang L, Xue C, Huang Z. Femtosecond laser-assisted deep anterior lamellar keratoplasty with big-bubble technique for keratoconus. Indian J Ophthalmol. 2016;64:639-642.
8. Ibrahim O, Elmassry A, Said A, Abdalla M, El Hennawi H, Osman I. Combined femtosecond laser-assisted intracorneal ring segment implantation and corneal collagen cross-linking for correction of keratoconus. Clin Ophthalmol. 2016;10:521-526.
9. Ganesh S, Brar S. Femtosecond intrastromal lenticular implantation combined with accelerated collagen cross-linking for the treatment of keratoconus—initial clinical result in 6 eyes. Cornea. 2015;34:1331-1339.
10. Pradhan KR, Reinstein DZ, Vida RS, et al. Femtosecond laser-assisted small incision sutureless intrastromal lamellar keratoplasty (SILK) for corneal transplantation in keratoconus. J Refract Surg. 2019;35:663-671.