



Treating dry eye disease (DED) is more complicated today than ever before. Gone are the days we could tell patients that they have DED without explaining the cause or the type. Today, we know that DED is multifactorial, and we know that it is crucial to treat the underlying cause—otherwise, our patients will not obtain lasting relief.
But how do we determine the cause, and what should we then do with that information? The answer is simple: We must use basic diagnostic principles to diagnose clinical features and guide treatment decisions. Here are five pointers for performing an effective DED workup.
No. 1: Talk, listen, and ask questions. A good diagnostic exam starts by simply talking to patients and listening carefully to what they say. Asking the right questions goes a long way in making a differential diagnosis. What are your chief complaints? Where does the eye feel most itchy? When do you commonly notice redness? These and other questions can help you to make a differential diagnosis even before doing any diagnostic testing.
No. 2: Look for signs of DED. It’s also very important to look at the patient to assess for signs of DED. Whether the patient blinks frequently or infrequently or whether the blinking is complete or incomplete can indicate tear film instability or a break in the tear film. Another simple task is to ask patients to look at a letter chart to determine how many letters they can read in one blink. If there is instability in the tear film, with this task their eyes will start to burn. This can certainly decrease the patient’s quality of vision.
No. 3: Look at the ocular surface as a system. Rather than looking at the ocular surface as separate structures such as the conjunctiva, cornea, and tear film, look at it as a system. This is important because the health of one structure can influence the entire system.
Let’s consider a patient with corneal damage. In looking at the entire ocular surface system and checking all its structures, you notice gland dropout and staining in the inferior parts of the cornea. In this case, the likely cause of that corneal damage is meibomian gland dysfunction, and, if you hadn’t considered the ocular surface as a system, you might not have come to that conclusion.
No. 4: Use vital dyes. This brings us to another key point in the diagnosis of DED: use of vital dyes. Vital dyes such as lissamine green and fluorescein are tremendously important.1,2 For starters, fluorescein dye can show punctate staining patterns related to DED and lagophthalmos, and it can be helpful when measuring tear breakup time and tear volume or checking for corneal decompensation. Use of fluorescein dye can also help to locate areas of corneal decompensation, whether in the inferior or central cornea or across 360º.
Lissamine green dye stains dead and degenerative cells (Figure). So in everyday practice we can diagnose inflammation of the ocular surface by simply using lissamine green dye.1,2 It is also helpful to assess the lid margin. If the lid margin line is irregular, the correct type of eyelid margin disease can be diagnosed. Lissamine green dye can also be used to stain the bulbar conjunctiva to see damage at that level, which can aide in the diagnosis of other ocular surface inflammatory diseases, such as limbal keratoconjunctivitis.
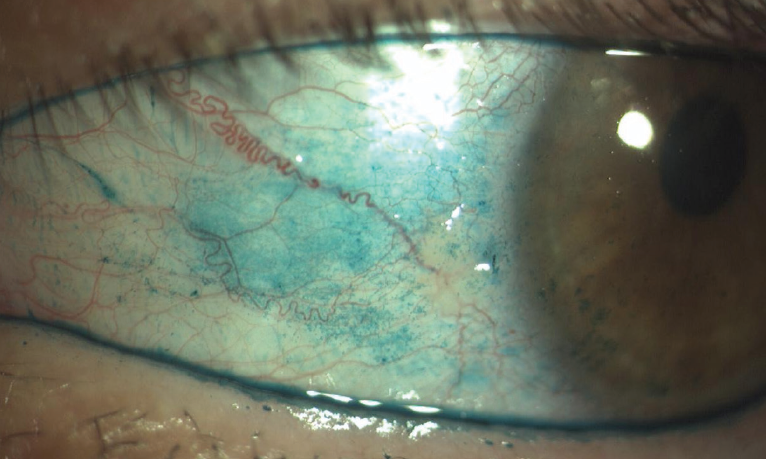
Figure. Ocular surface staining with a new formulation of lissamine green (Lissagreen, Polifarma). The conjunctival staining in the eye correlates with ocular surface inflammation indicative of chronic dry eye. This eye was treated with topical antiinflammatory drops.
No. 5: Consider the inflammation. Careful consideration of the inflammatory component of DED is essential. A variety of systems can be used to measure ocular surface inflammation, but all have limitations. A combination of impression cytology to collect cells with measurement of inflammation markers and flow cytometry is the most effective technique to quantify the level of inflammation on the ocular surface. Unfortunately, the procedure has limitations, including high cost and the need to collaborate with an immunology laboratory or other facility with a flow cytometer. Other methods include matrix metallopeptidase-9 (MMP-9) evaluation and measurement of tear osmolarity. MMP-9 testing is easy to perform, but it provides only qualitative results. Tear osmolarity is an indirect marker of inflammation, and its pros and cons have been described in the literature.
CONCLUSION
Using even basic diagnostic principles like questioning and observing the patient’s habits, staining the ocular surface with vital dyes, and considering the inflammatory component of DED can be extremely helpful in guiding effective treatment of DED.
1. Yang S, Lee HJ, Kim DY, Shin S, Barabino S, Chung SH. The use of conjunctival staining to measure ocular surface inflammation in patients with dry eye. Cornea. 2019;38:698-705.
2. Hamrah P, Alipour F, Jiang S, Sohn JH, Foulks GN. Optimizing evaluation of lissamine green parameters for ocular surface staining. Eye. 2011;25:1429-1434.