


In complex and challenging cases, the pre- and intraoperative courses must be carefully planned and executed to ensure the best possible outcomes for our patients. In many cases, this entails deciding between surgical approaches by considering the pros and cons for each of them. The case described here and in the accompanying Eyetube video is no exception.
CASE REPORT
A hypertensive 84-year-old pseudophakic patient was referred for corneal transplant in the right eye—his only functional eye. (The patient’s left eye had no light perception due to advanced glaucoma and a corneal leucoma through which no detail could be seen.) The patient’s visual acuity was counting fingers at 50 cm OD, with good light perception in all quadrants. At the slit lamp, the cornea showed diffuse edema in all layers with epithelial bullae. The IOL was in the capsular bag, and inferonasal subluxation of the IOL and capsular bag complex and severe pseudophacodonesis were noted. The pupil dilated with mydriatics only to 4 mm, and pseudoexfoliative material was present at the pupil margin. The anterior capsule appeared fibrotic and contracted (Figure 1). IOP by palpation was about 30 mm Hg, and the patient was under treatment with travoprost.
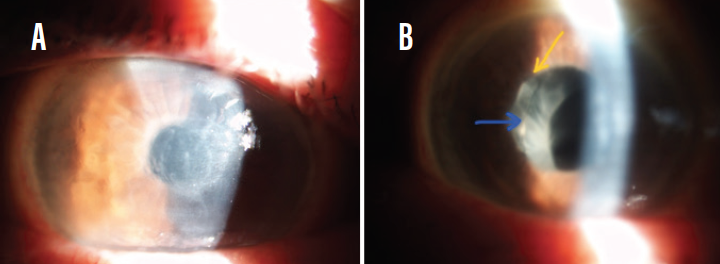
Figure 1. At the slit lamp, the cornea showed diffuse edema in all layers with epithelial bullae (A); the anterior capsule appeared fibrotic and contracted (arrows; B).
Anterior segment OCT (AS-OCT) documented a thick cornea (740 µm) and large iridocorneal angle in the right eye. B-scan ultrasound revealed an attached retina, a posterior vitreous detachment, and no visible sign of enlarged cup-to-disc ratio. Ultrasound biomicroscopy (UBM) with the patient in supine position showed moderate to severe posterior dislocation of the IOL and capsular bag (Figure 2).

Figure 2. UBM with the patient in supine position showed moderate to severe posterior dislocation of the IOL and capsular bag.
A fixed combination of dorzolamide HCl/timolol maleate was added to the patient’s glaucoma regimen. When he was reevaluated 3 weeks later, IOP was about 20 mm Hg OD. After seeing this good response to treatment, we scheduled the patient for combined surgery.
SURGICAL DECISION-MAKING
The combination of several morbidities in this patient’s only functional eye made this case challenging, requiring complex preoperative evaluation and discussion in order to determine the best surgical technique to offer this patient.
Pseudoexfoliation syndrome (PEX) is a known cause of late posterior chamber IOL dislocation, often associated with pseudoexfoliative glaucoma. The IOL is usually well fixated and centered in the capsular bag at the time of cataract surgery, but, due to zonular laxity and later breakage of zonular fibers, the whole complex of the capsular bag and IOL loses its normal central retropupillary position over time and becomes subluxated in the anterior or posterior vitreous.
Patients present with pseudophacodonesis in early stages, but later stages include inferior dislocation of the IOL with appearance of the IOL optic margin in the pupil. Eventually no IOL or bag are visible in the pupil, and the complex is completely luxated into the posterior segment. B-scan ultrasound examination of the posterior pole and UBM can reveal the degree of the IOL dislocation and its position in the eye.
Cataract surgery in eyes with PEX is always challenging; poor pupil dilatation and zonular laxity make the surgery difficult and prone to intraoperative complications. These eyes can develop dislocation of the IOL and bag years after uncomplicated cataract surgery, requiring repositioning in order to improve the patient’s visual acuity and avoid further complications. When bullous keratopathy is associated, the surgery becomes even more challenging.
Several options have been proposed for approaching these eyes, and each has advantages and drawbacks.1-4 Suturing a dislocated four-haptic posterior chamber IOL within the bag has been described,5-7 but, to the best of our knowledge, none were cases performed with concurrent posterior lamellar keratoplasty.
PLANNING A STEPWISE APPROACH
In the case described here, we had to decide between a stepwise approach, with separate surgical events for corneal transplant and IOL repositioning, or the combination of both in a single procedure. The type of corneal transplant—penetrating keratoplasty (PKP) or endothelial keratoplasty (EK)—and the modality of dealing with the decentered IOL were also part of the debate. Moreover, whether to perform glaucoma surgery as a separate procedure, combined in a triple procedure, or at all was also discussed.
In our case, apart from the ocular comorbidities and the type of IOL already implanted, other factors had to be considered, including the patient’s advanced age and associated systemic diseases. First, the decrease in IOP to a normal level with the addition of only one topical medication, with presumed satisfactory cup-to-disc ratio (as evaluated through B-scan and medical records), correlated with the patient’s age and life expectancy, led us to eliminate the glaucoma surgery component at that time. We also excluded the two-step approach because of the higher physical and psychological stress this would entail for the patient, who asked only to see with his right eye as soon as possible for “what is left of my life.”
We also decided against IOL and bag explantation with implantation of a new IOL because of the associated greater trauma and higher costs. Moreover, we did not consider the implantation of any type of anterior chamber IOL due to the threat it would pose to the corneal graft. Given all this, we decided to reposition the existing IOL and bag and to perform the corneal transplant in the same surgery.
What technique, then, would we use to reposition the IOL? Because the slit-lamp examination revealed a part of one haptic, showing a thick acrylic loop, neither scleral tunnel insertion nor the Yamane technique would be suitable. Thus, suturing the existing IOL was the only option.
PKP and suture of the IOL and bag to the sclera. The pros of this technique include easier surgery, with direct visualization of the eye structures and enough room for maneuvers; however, it comes with high risk for expulsive hemorrhage in a prolonged open sky surgery for a hypertensive patient.
EK with IOL and bag complex sutured to the sclera under pars plana infusion, with limited pars plana vitrectomy.In this technique, the advantages include that it is a safer, closed-eye procedure. Yet it would be a more difficult and expensive technique, requiring a vitreoretinal surgeon.
EK with IOL and bag sutured under an anterior chamber maintainer, with local vitrectomy through the anterior route.If this technique was chosen, it is true that it would be a safer, closed-eye procedure with an anterior approach. It is also easier and less expensive to perform than some of the other procedures; however, it could be difficult to capture the IOL if it is found to be dislocated too far posteriorly.
PKP was eliminated due to its higher intraoperative risks. Further, Descemet membrane EK was avoided because it is a longer procedure and because the probability of postoperative graft detachment would have been high in this eye. Thus, Descemet-stripping automated EK (DSAEK) with an anterior approach was chosen, for the reasons I enumerated previously.
SURGICAL TECHNIQUE
The first part of surgery addressed the suturing of the IOL and capsular bag. This was accomplished with an anterior segment approach under an anterior chamber maintainer. The epithelium was first removed to allow better visualization.
Two 3-mm scleral grooves were made at 2 mm posterior to the limbus and parallel to it, 180° apart. Iris hooks were inserted to enlarge the pupil so that the haptics could be visualized. Then the dislocated bag was grasped with vitreoretinal forceps and two of the hooks were repositioned from the iris to the continuous curvilinear capsulorhexis (CCC) to stabilize the bag during haptic suturing (Figure 3).

Figure 3. The inferior hooks grasp the CCC, stabilizing the bag, while the superior hooks are fixed on the iris, providing visualization of the superotemporal haptic.
The visible haptic was sutured with double-armed 9-0 polypropylene suture using an ab-externo technique (Figure 4A and 4B), leaving both ends of the suture exposed through the corresponding scleral groove. The same maneuver was then completed for the opposite haptic, after repositioning the other two hooks from the iris to the CCC and the first two hooks back onto the iris, to provide better pupil enlargement in this new area of interest (Figure 4C and 4D). A video of this step of the procedure can be viewed at bit.ly/moraru0420.
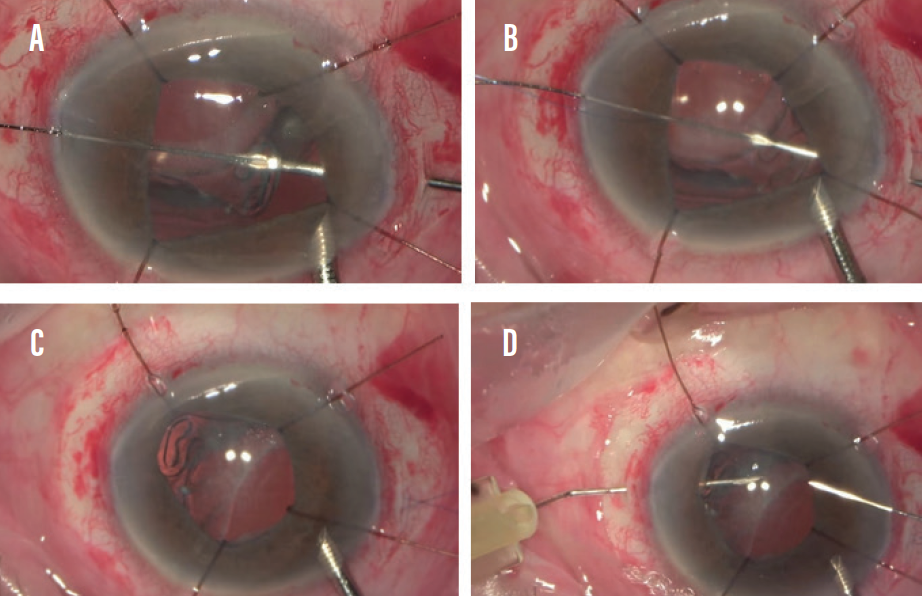
Figure 4. Ab-externo technique for suturing the superotemporal (A, B) and inferonasal (C, D) haptics.
Finally, both sutures were exposed in both scleral grooves. Then, by pulling them with equal tension, the IOL and bag became centered and stabilized (Figure 5). The sutures were tied and the knots buried in the scleral grooves. The focus then turned to the corneal transplant surgery. This would be a standard DSAEK, with graft lamella prepared by the surgeon with a microkeratome on an artificial anterior chamber. After performing descemetorhexis and peripheral iridotomy, the graft was implanted and an air bubble placed underneath it with moderate pressure.

Figure 5. Both sutures are exposed symmetrically in the scleral grooves. By pulling them with equal tension, the IOL and bag became centered and stabilized.
POSTOPERATIVE OUTCOME
On the first postoperative day, the graft looked transparent and attached at the slit lamp, the anterior chamber had a small air bubble, the IOL was centered in the pupil, and the IOP was about 10 mm Hg. AS-OCT showed a tiny detachment of the graft margin at the 8 to 9 clock positions (Figure 6A).
On day 2, the graft looked more edematous and there was no air bubble in the anterior chamber. AS-OCT showed progressive detachment of the lamella (Figure 6B), so it was decided to re-bubble, after which the lamella remained completely attached (Figure 6C).
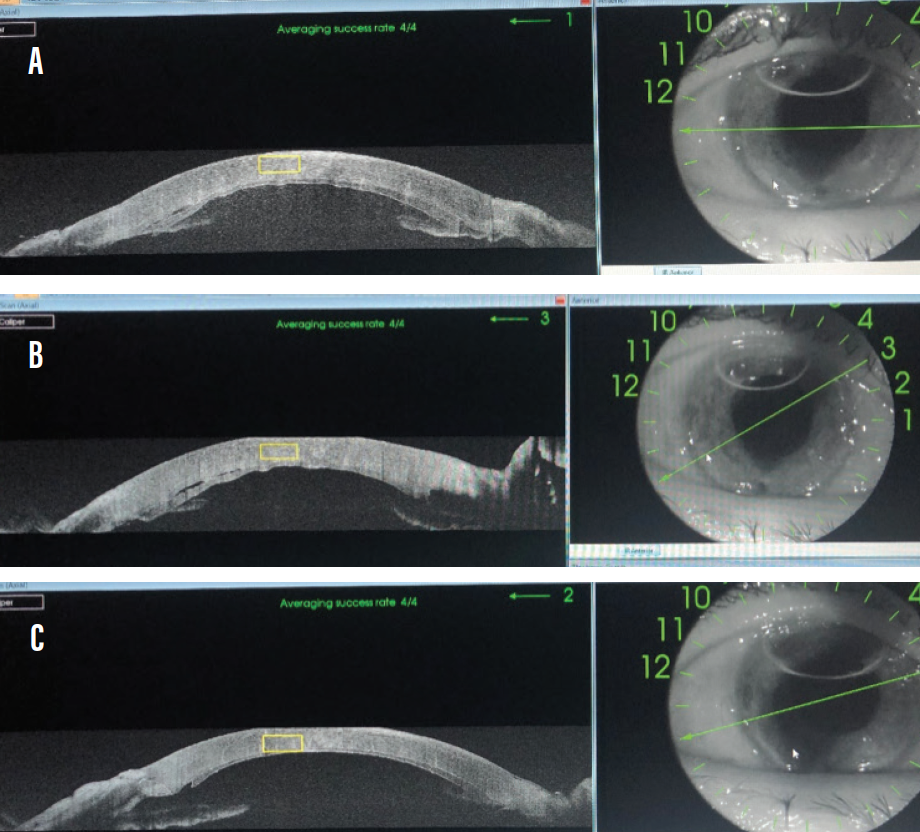
Figure 6. AS-OCT on postoperative days 1 and 2 (B) and on postoperative day 2 after re-bubble (C).
At 5 days postoperative, the graft was transparent and the IOL well centered (Figure 7A and 7B). At 1 month postoperative, the distance UCVA OD was 20/100 Snellen, IOP was 19 mm Hg with medication, the graft was thin and transparent, and the IOL was well centered in the bag and in relation to the pupil. AS-OCT showed a completely attached graft 95 µm thick.

Figure 7. Slit-lamp appearance (A) and UBM (B) at postoperative day 5, which was 3 days after re-bubble.
The patient will continue with the topical treatment (travoprost and timolol maleate). Follow-up visits are scheduled to evaluate the cornea and to closely monitor the glaucoma.
CONCLUSION
In this complex and challenging case, the intra- and postoperative courses were uneventful, except for a minor peripheral graft detachment due to poor persistence of the anterior chamber air bubble necessitating one re-bubble. After that, we obtained good graft reattachment and anatomic rehabilitation.
We expect favorable short-term results for this patient, but long-term graft survival and visual acuity preservation will depend heavily on the control of the glaucoma in this patient’s lone functional eye.
1. Subasi S, Yuksel N, Karabas VL, Yilmaz Tugan B. Late in-the-bag spontaneous IOL dislocation: risk factors and surgical outcomes. Int J Ophthalmol. 2019;12(6):954-960.
2. Fernández-Buenaga R, Alio JL, Pérez-Ardoy AL, et al. Late in-the-bag intraocular lens dislocation requiring explantation: risk factors and outcomes. Eye (Lond). 2013;27(7):795-801.
3. Khan MA. Management options for dislocated intraocular lens. Retinal Physician. June 2018.
4. Stem MS, Todorich B, Woodward MA, Hsu J, Wolfe JD. Scleral-fixated intraocular lenses: past and present. J Vitreoretin Dis. 2017;1(2):144-152.
5. Ivanova NV, Rasin OG, Savchenko AV, Litvinenko OA, Ogbonna GW. Clinical results of vitrectomy with the fixation of the intraocular lenses Akreos AO60 to the sclera. MedCraveOnLine Journal of Surgery. 2017;5(2):185-187.
6. Aderman CM. Four-point fixation for scleral-sutured IOLs. Retina Today. March 2018.
7. Khan MA, Gupta OP, Hsu J. Scleral fixation of a four-haptic intraocular lens using Gore-Tex suture. Retina Today. November/December 2015.
