
Refractive surgery has a rich history. In 1975, Krasnov introduced the concept of photodisruption of ocular tissue with short laser pulses in the nanosecond and picosecond range.1 The energy required for the laser pulses at the time, however, led to mechanical side effects, mainly bubble formation, which prevented successful completion of the procedure. Over time, incremental improvements in laser technology, especially in the shortening of pulse durations to femtoseconds made it possible to overcome the obstacle of high pulse energy, making refractive corneal surgery a reality.
Today, femtosecond laser systems are routinely used to perform lens and corneal-based procedures, including lenticule extraction. I have been involved with the development of lenticule extraction since the early days of the technique and have published extensively on the topic of lenticule extraction with a low energy laser system.2-4 This article describes the multiple advantages of low energy and provides a brief history of lenticules.
BACKGROUND
Just before the turn of the millennium, in 1998, our group began to experiment with intrastromal refractive surgery and the idea of lenticule extraction (Figures 1 and 2). I remember being inspired by the early work of Kurtz and Juhasz, who in 1997 showed that femtosecond lasers could be used to cut tissue below the cornea much more precisely than picosecond lasers.5 Their work was so exciting because many of us were looking for alternatives to ablation with excimer lasers. Some colleagues tried to use the erbium laser for ablation, which was cheaper and smaller, but the results were not as good as what excimer lasers could produce. The need for better procedures in refractive surgery was clear.
Figure 1. Professor Lubatschowski’s first publication on intrastromal refractive surgery and lenticule extraction in 1999.2
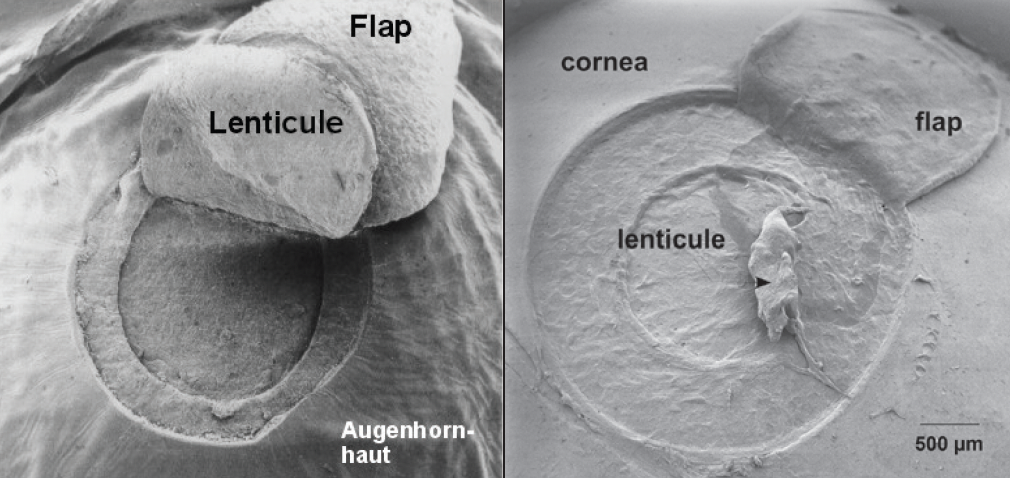
Figure 2. Scanning electron microscopy of one of the first flaps and lenticules created in a pig eye at 1.2 μJ pulse energy (1998).
Their idea to use ultrashort pulses to cut tissue below the surface was literally disruptive and at the same time right under our noses—for some time, femtosecond lasers were used in our laboratories to process glasses. It did not take long for the ophthalmic industry to recognize the advantages of intrastromal refractive surgery, and several manufacturers began to develop femtosecond lasers that could be used to perform refractive procedures below the corneal surface. The first generation lasers used a comparatively high pulse energy to generate the cutting process.
Several of my colleagues and I saw it as a scientific challenge to take the concept of intrastromal disruption that was established in the literature and optimize the process. We knew that extremely short pulse duration and focal volume (ie, spot size) could still produce very high intensities with the application of low energy only, and we postulated that it could be used to create a lenticule that could achieve refractive correction.
In 1999, we presented our concept for low-energy intrastromal refractive surgery at several conferences and wrote and published many studies. The first peer-reviewed paper was published in Graefes Archive for Clinical and Experimental Ophthalmology in 2000.4 Thereafter, we partnered with Ziemer in the development of a laser system that could separate tissue with the lowest amount of pulse energy not reached by any other laser system. This was possible due to a handpiece design from Ziemer with specially developed microscope optics with a very short focal distance (Figure 3).
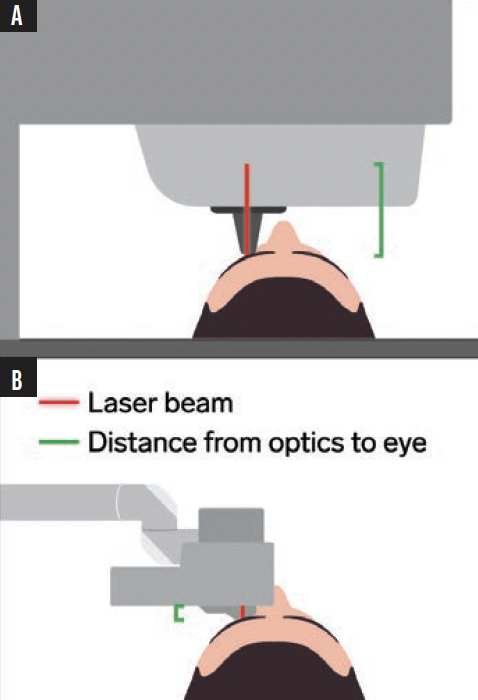
Figure 3. Conventional femtosecond lasers without a handpiece (A) have a long working distance to the eye whereas the small handpiece of Ziemer works from a short distance (B).
INTRODUCTION OF THE FEMTO LDV
In 2005, the FEMTO LDV (Ziemer) became commercially available. This device was smaller than other femtosecond lasers, and it had a lower pulse energy and higher repetition rate, which has many advantages over higher pulse energy femtosecond lasers. Higher pulse energy causes unwanted mechanical side effects like tissue rupture, cavitation, shockwaves, and bubble formation that can lead to opaque bubble layers in the stromal tissue. Lower pulse energy, on the other hand, helps to protect the adjacent ocular tissue and produces higher precision. Last but not least, low-energy pulses can also be generated using a much more compact and robust laser system that promises true mobility.
Because the cutting process with a low pulse energy laser is naturally slower than lasers that use high pulse energy, an increase in the repetition rate is required to achieve a similar cutting rate. The current FEMTO LDV Z8 platforms operate with a repetition rate of up to 20 MHz. Further, the small spot size and overlapping spots delivered with the Ziemer laser produce complete tissue dissection and eliminate tissue bridges. The FEMTO LDV is therefore, by design, the most precise laser for cutting cornea. As a result, new applications with higher precision requirements—such as the creation of lenticules—can be easily installed via software. No hardware modification is required.
The FEMTO LDV is designed with a flat patient interface for most corneal surgeries. Combined with a controlled vacuum system, this provides maximum precision and control over the patient’s eye. Suction loss is therefore not an issue.
THE INTRODUCTION OF LENTICULE EXTRACTION
LASIK is a well-established procedure. The ablation is extremely precise—it is one-quarter of a micrometer per pulse—and the way in which ocular tissue reacts to an excimer laser ablation is well known. A flapless, intrastromal refractive procedure such as lenticule extraction, however, is attractive to surgeons and patients alike because it avoids some of the challenges associated with LASIK, including flap-related complications and the risk for dry eye disease postoperatively.
The lenticule extraction procedure only requires a small keyhole incision through which the lenticule can be removed. The lenticule extraction application is available as a software upgrade to the FEMTO LDV Z8 and FEMTO Z8 NEO, both of which can also be used to perform cataract surgery, LASIK, tunnels for rings, pockets for inlays, and keratoplasty procedures.
CONCLUSION
Lenticule extraction is an exciting evolution in the history of refractive surgery. The procedure is currently indicated for myopic correction, and future applications are in development.
The future of femtosecond laser applications in ophthalmology is low energy, and Ziemer is blazing the trail.
1. Krasnov MM. (aser-phakopuncture in the treatment of soft cataracts. Br J Ophthalmol. 1975;59(2):S96-98.
2. Lubatschowski H, Maatz G, Heisterkamp A, Welling H, Ertmer W. Intrastromal refractive surgery by fs laser pulses. In: Biomedical Optics. OSA Technical Digest. Optica Publishing Group. 1999; Paper CMA2.
3. Heisterkamp A, Maatz G, Ripken T, et al. Intrastromal refractive surgery by ultrashort laser pulses: side effects and mechanisms. SPIE Proceedings Ophthalmic Technologies X. 2000.
4. Lubatschowski H, Maatz G, Heisterkamp A, et al. Application of ultrashort laser pulses for intrastromal refractive surgery. Graefes Arch Clin Exp Ophthalmol. 2000:33-39.
5. Liu X, Kurtz RM, Braun A, Liu H, Sacks Z, Juhasz T. Intrastromal corneal surgery with femtosecond laser pulses. In: Conference on Lasers and Electro-Optics. Killinger D, Valley G, Chang-Hasnain C, Knox W, eds. OSA Technical Digest. Optica Publishing Group. 1997;11:CTuT5.
