
The most common method for opening the anterior lens capsule during cataract surgery is by continuous curvilinear capsulorhexis. This technique provides excellent structural integrity of the capsular bag, and it is resistant to peripheral extension during subsequent maneuvers of the procedure, including nucleus manipulation, cortical removal, and IOL implantation. Other alternatives, however, can be advantageous in specific surgical situations. High-frequency (HF) capsulotomy with the OS 4 Surgical platform (Oertli Instrumente AG, Switzerland) is a versatile and gentle alternative, especially in the setting of high intracapsular pressure such as in eyes with loose or weak zonules, hypermature and intumescent cataracts, pediatric cataracts, small pupils, excessive shrinking of the capsular bag, and conditions for which there is no red reflex (Figure 1).
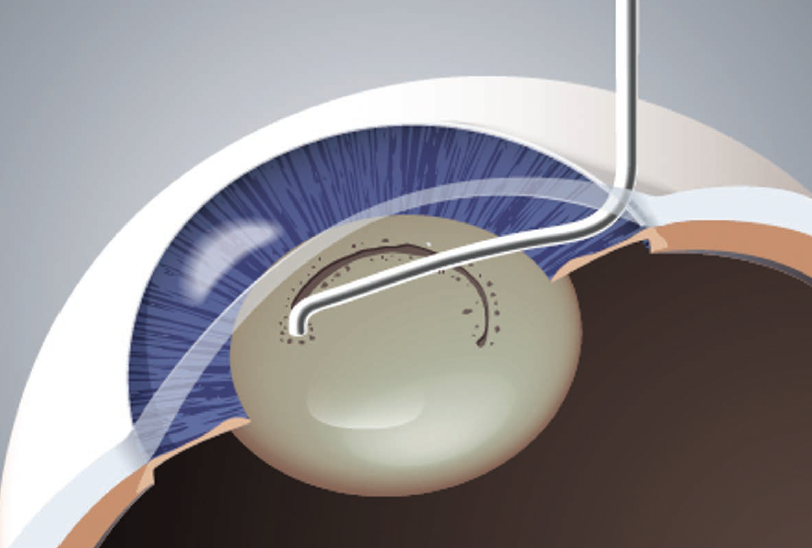
Figure 1. HF capsulotomy is a gentle alternative to the continuous curvilinear capsulorhexis.
WHAT IS HF CAPSULOTOMY?
Capsulotomy with high-frequency energy is a proven technique that has been used for many years. In short, high-frequency diathermy is used to gently melt the capsular bag without any tearing with forceps and needles. The anterior capsule opens reliably and in a controlled fashion, resulting in a well-centered capsulorhexis of the right size and shape. The capsulotomy tip simply slides gently over tissues and under the iris tissue with an extremely fine and directly controllable dosing of high-frequency energy. The edge of the HF capsulotomy is structurally sound and of the highest quality from the moment it is created and extending into the postoperative period.
The only tools required for HF capsulotomy include a short or long diathermy handpiece (both by Oertli Instrumente AG, Switzerland) and a standard or extended reusable capsulotomy tip (both by Oertli Instrumente AG). In my experience, both the short and long diathermy handpieces are very ergonomic, and the tips attach to the handpiece with a simple plug-in motion (Figure 2). It also has a long cable (3 m), which allows easy maneuverability.
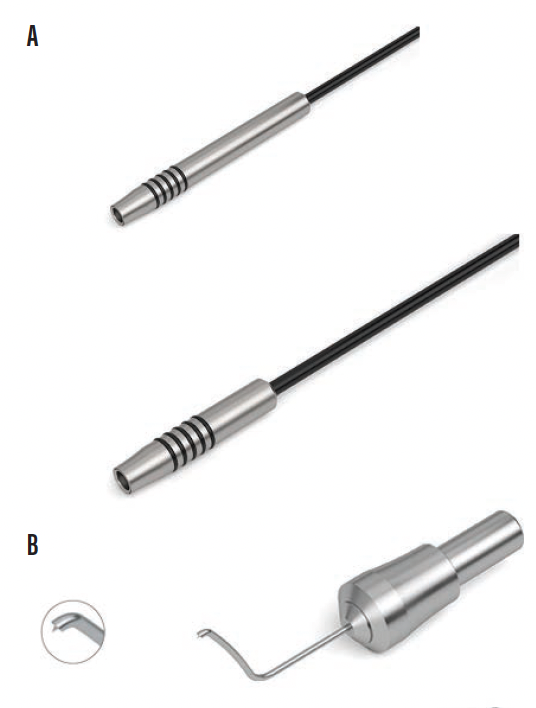
Figure 2. Equipment required for HF capsulotomy includes any Oertli phaco platform, long or short diathermy handpiece (A), and capsulotomy tip (B).
Both capsulotomy tips can fit easily through the main incision. I recommend the use of OVD when inserting either tip through the incision. Another alternative is to use irrigation through the main incision while inserting the HF capsulotomy tip through the paracentesis.
Typically, I perform HF capsulotomy with an energy of 500 kHz. For denser cataracts, however, I will increase the energy up to 600 kHz as needed. Histopathological and scanning electron microscopy investigations have shown that the edge of the HF capsulotomy is very tight, firm, and resistant to tearing. Additionally, a capsular tension ring or capsular tension segments can be implanted safely with a HF capsulotomy.
TIPS AND TRICKS
HF capsulotomy is not a new technique, but several tips and tricks are equally helpful for those with and without experience performing this procedure. These pointers can help one to individualize the capsulotomy according to the needs of the specific case.
No. 1: Before performing HF capsulotomy, pass over the entire anterior chamber to the angle of the other side with the leading cannula before injecting the OVD. This removes all of the fluid from the anterior chamber to ensure a homogenous fill of the OVD.
No. 2: Puncture the anterior capsule with the capsulotomy tip while applying energy with the footpedal of the OS 4. During this maneuver (Figure 3), the fluid will egress through the paracentesis. A small bolus of OVD can also be injected during this step and the energy increased slightly. The greater the energy, the greater the effect.
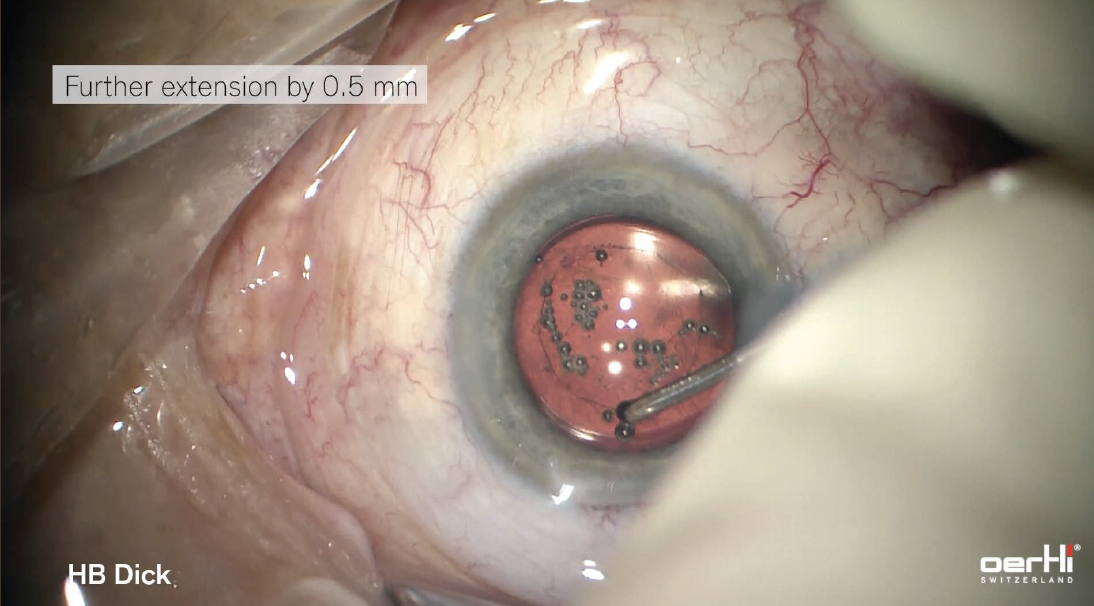
Figure 3. The HF capsulotomy is created under the surgeon's full control.
No. 3: Start small. One advantage of a HF capsulotomy is that the surgeon can start by creating a smaller capsulotomy and enlarging it after IOL implantation, as needed, based on the position of the lens. This is especially important in pediatric eyes because these eyes have more retraction forces than normal age-related cataracts do. The goal is to achieve a 360º overlap of the anterior capsule and the IOL to avoid capsular fibrosis and lens decentration. I prefer to start with a 4.3- to 4.4-mm capsulotomy. Enlargement can be achieved easily with the HF capsulotomy tip, reentering the eye to reshape the capsulorhexis.
No. 4: Gas bubbles are normal. During the creation and/or enlargement of the HF capsulotomy, the presence of gas bubbles is completely normal (Figure 4). They form as a result of the heat from the diathermy tip.
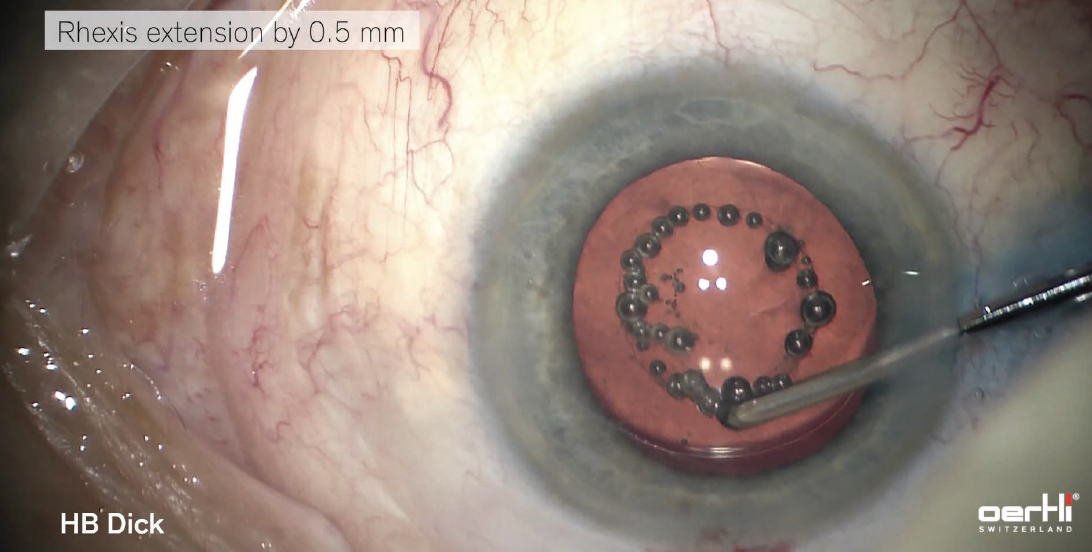
Figure 4. The presence of gas bubbles is normal.
No. 5: Polish the capsule. The cortex can adhere to the underside of the anterior capsule. To avoid this, meticulous polishing of the entire capsular bag is therefore recommended after IOL implantation.
CONCLUSION
HF capsulotomy is a well-established technique that has been in our armamentarium for many years. It’s an excellent alternative to the continuous curvilinear capsulorhexis, especially for cases in which the intracapsular pressure is high. This great technology continues to be relevant today, and surgeons of all experience levels can master the technique. The anterior capsule is opened gently and in a controlled fashion without any tearing with forceps and needles. HF capsulotomy is just another way that we can individualize patient care and help patients achieve excellent postoperative outcomes.



