




Cataract surgery has become a refractive procedure, as it goes beyond the simple restoration of sight. Surgeons now seek to provide patients with a wide range of excellent visual acuities at different distances, along with high optical quality and improved contrast sensitivity. The portfolio of commercially available multifocal IOLs and enhanced depth of focus (EDOF) IOLs offers a wide range of options to surgeons, especially regarding the materials used and their optical profiles.
The availability of such IOL models not only offers the option of presbyopia correction in routine cataract surgery; it also helps us to individualize patient care. To choose the right presbyopia-correcting IOL, surgeons must consider the importance of each patient’s daily activities and assess his or her degree of tolerance of possible dysphotopsias. Additionally, the IOL optic design and the patient’s ocular physiology are major factors in determining the appropriateness of a given IOL model. It is a communication-based decision that depends on proper counseling and adequate chair time.
The aim of this article is to describe five modern classes of presbyopia-correcting IOLs, differentiated by the mode of action due to the optical design, the optical profile, and the addition power on the lens base. We will also discuss how we consider patients’ demands and lifestyles in choosing the best IOL for each one’s needs and expectations.
Fundamental 1: High-add bifocal IOLs are beneficial for patients who do near work
Some ophthalmologists no longer consider high-add bifocal IOLs to be state of the art, but there is a certain population of patients for whom sharp near vision at a close distance of approximately 30 cm is necessary. This includes patients who primarily perform activities at distances closer than 40 cm, such as fine needle work or intensive reading.
The multifocality of high-add lenses offers very good far and near visual acuities, but it comes at the cost of a sudden dropoff in intermediate vision and the perception of halos and glare, especially in IOLs with diffractive optical profiles. However, multiple studies have shown high patient satisfaction when these IOLs are implanted in the right patients who accept that they will need spectacles for intermediate vision.1-3
High-add bifocal IOLs generally come with adds between 3.00 and 4.00 D. Exceptions include the Scharioth Macula Lens (Medicontour), a bifocal lens with a special central optic providing a high addition of 10.00 D, and the Lentis LS-313 MF80 (Oculentis), a rotationally asymmetric refractive multifocal IOL with a near-add power of 8.00 D at the IOL plane that works as a magnifying glass. These IOLs were developed for low-vision patients with dry age-related macular degeneration, but they have proven to be useful in patients with other macular diseases, too. They provide magnified vision for a very near distance (approximately 10 to 15 cm) while preserving distance vision.
The choice of specific IOL and add depends on the distance that the patient requires for his or her activities, as well as the surgeon’s preferences concerning material and optical profiles.
Examples of High-Add Bifocals IOLS
- AcrySof ReStor SN6AD1 +3.0 D and SN6AD3 +4.0 D IOLs (Alcon); near adds 3.00 and 4.00 D, respectively
- Lentis Mplus LS-313MF30 (Oculentis; Figure 2); >near add 3.00 D
- Tecnis ZLB00 and ZMB00 (Johnson & Johnson Vision); near adds 3.25 and 4.00 D, respectively
- Diffractiva (HumanOptics); near add 3.50 D
- Scharioth Macula Lens (Medicontour); near add 10.00 D
- Zeiss AT LISA 809 (Carl Zeiss Meditec); near add 3.75 D
- Lentis LS-313 MF80 (Oculentis); near add 8.00 D
Case report. A presbyopic 73-year-old woman with bilateral age-related nuclear cataract reported that she loves reading history books and knitting. She rarely uses a computer or other devices, and she does not mind using spectacles for intermediate vision. She wants to achieve spectacle independence for near vision. At her preoperative visit, the patient’s refraction was +2.75 -0.25 × 71° OD and +3.25 -1.00 × 93° OS, and her BCVA was 0.3 logMAR in each eye.
We chose to implant the Tecnis ZMB00 with a 4.00 D add (Johnson & Johnson Vision) IOLs bilaterally.3 We calculated the IOL power with the IOLMaster 700 (Carl Zeiss Meditec) using the Barrett Suite to be 24.00 D in both eyes, targeted for emmetropia. This provided the patient with excellent far and near visual acuities. Postoperatively, she achieved distance and near UCVAs of 0.0 logMAR and is happy with her outcome.
Fundamental 2: Trifocal IOLs meet the need for intermediate vision
Patients increasingly express a desire for good intermediate vision due to the growing use of computers and devices. This has led to the development of trifocal IOLs by multiple manufacturers. The first to be introduced, the FineVision IOL (PhysIOL),4,5 combined two diffractive bifocal profiles, one for near and far distance and the other for intermediate and far distance at half the dioptric power of the former, thus creating a third, harmonized focus.
This design provides patients with a wider range of vision and more spectacle independence, but some patients can complain about dysphotopsia, although with less frequency and lower intensity than with bifocal IOLs.
Deciding which patients are candidates for these lenses depends enormously on chair time and the counseling process. Counselors must spend time with patients in order to select the most suitable IOL to meet their needs and to set the right balance between their tolerance of dysphotopic phenomena and their desire for spectacle independence at different distances. Patients who are motivated, who live an active lifestyle that requires intermediate vision, and who are tolerant of dysphotopsia in mesopic conditions are perfect candidates for trifocal IOLs. Several studies have shown the ability of trifocal IOLs to provide excellent visual acuity, spectacle independence in different distances, and patient satisfaction with the outcomes of the surgery.4-12 This can be achieved only if patients are correctly counseled preoperatively.
Examples of Trifocal IOLS
- AT LISA tri (Carl Zeiss Meditec); near add 3.33 D, intermediate add 1.66 D
- FineVision Pod F and Micro-F (PhysIOL); near add 3.50 D, intermediate add 1.75 D
- PanOptix (Alcon); near add 3.25 D, intermediate add 2.17 D
- RayOne trifocal (Rayner); near add 3.50 D, intermediate add 1.75 D
- Acriva Trinova trifocal (VSY Biotechnology); near add 3.00 D, intermediate add 1.50 D
Case report. A 70-year-old woman with bilateral age-related nuclear cataract was counseled regarding her expectations from cataract surgery. Her refraction was +2.75 -1.00 × 93° OD and +3.25 -1.25 × 3° OS with distance BCVAs of 0.6 logMAR OD and 0.3 logMAR OS preoperatively.
She stated that she would like to achieve as much spectacle independence as possible at all distances. We suggested bilateral implantation of the trifocal AT LISA tri 839 MP (Carl Zeiss Meditec)5,8-11 and informed the patient about the possibility of photic phenomena. Targeting emmetropia, the IOL powers were 23.50 D OD and 25.00 D OS.
At the 3-month postoperative visit, the patient presented distance, intermediate, and near UCVAs of -0.1 logMAR OD and 0.0 logMAR OS. She was very satisfied with the outcomes of the surgery, with her vision, and especially with her spectacle independence at all distances.
Fundamental 3: Diffractive EDOF IOLs provide an extended range of vision with less photic phenomena
After the development of trifocal lenses, innovations were directed toward attempts to enhance range of vision while decreasing photic phenomena. The concept was to make an IOL that produces less dysphotopsia, better contrast sensitivity, and good visual acuity at a continuous range of vision instead of at distinct specific foci, which can leave patients with blurry vision in between focal points.
EDOF IOLs attempt to meet these demands; there are several on the market that have shown good results. The first diffractive EDOF was the Tecnis Symfony (Johnson & Johnson Vision),13-15 followed more recently by the AT LARA 829MP (Carl Zeiss Meditec).16 These EDOF IOLs allow an extended range of vision from far to intermediate distance (within an arm’s length, approximately, from the eye). They are suited to patients who have little tolerance for dysphotopsia but do not mind the occasional use of spectacles for reading small print.
Examples of EDOF IOLS
- Tecnis Symfony (Johnson & Johnson Vision)
- AT LARA 829MP (Carl Zeiss Meditec)
Case report. A 51-year-old woman with bilateral age-related nuclear cataract and hyperopia in both eyes was counseled in our outpatient department for cataract surgery. Her refraction was +4.00 -0.25 × 85° OD and +4.25 -0.50 × 106° OS. During the counseling visit, she related that she uses a computer almost 8 hours a day in her job as an account manager. The patient drives at night frequently as part of her daily commute and would like to have the least possible photic phenomena. She does not mind using spectacles for near activities such as reading her book at night, as she already keeps a pair of reading glasses on her nightstand. At the time of her first visit, the patient had a distance BCVA of 0.2 logMAR, and Pentacam (Oculus Optikgeräte) keratometry (K) measurement revealed a flat axis K1 of 41.00 and 40.90 D and a steep axis K2 of 41.00 and 41.80 D in the patient’s right and left eyes, respectively.
We chose to implant bilateral AT LARA EDOF IOLs, and we calculated the IOL power with the IOLMaster 700, using the Barrett Suite, as 30.00 D in her right eye and 31.00 D in her left.
At the 1-month postoperative visit, the patient’s distance UCVA was -0.09 logMAR, with a continuous range of visual acuity of -0.02 logMAR from far to 60 cm distance. The Figure shows the patient’s monocular and binocular defocus curves. Even though she experienced moderate photic phenomena that she described as “a little bothersome,” she was satisfied with the results of the surgery and the choice of the IOL.
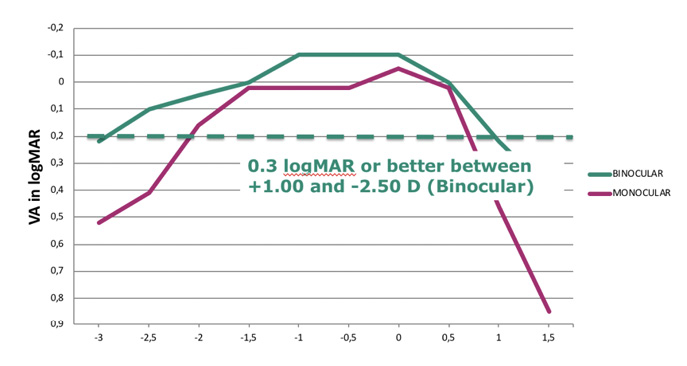
Figure. Monocular (green) and binocular (magenta) defocus curve after implanatation of the AT LARA 829 MP.
Fundamental 4: The pinhole EDOF IOL is intended to improve near vision based on the concept of small-aperture optics
The small-aperture EDOF IOL concept is similar to the principle of a pinhole camera. It cuts off light rays that do not pass through its central aperture, resulting in a dimmer image but with increased depth of focus. The IC-8 (AcuFocus) is the only IOL on the market using this technology. It features a central annular mask and was inspired by the company’s Kamra corneal inlay. It is an interesting option for patients with irregular corneas, such as those caused by traumatic injuries.
The IOL allows central rays to pass through the aperture while limiting peripheral rays that can affect focus and cause glare in certain cases. The lens is forgiving in terms of visual acuity in patients with residual astigmatism or deviations from target refraction. It is also a good option for presbyopic patients, although photic phenomena are an issue, especially in patients with large mesopic pupil sizes.
xample of Pinhole EDOF IOL
- IC-8 (AcuFocus)
Case report. A 6-year-old boy presented with slow progressive vision loss in his left eye over the previous 2 years. He had been diagnosed with posterior synechia and congenital cataract at the age of 1. Visual acuity was 0.5 logMAR OD with anisometropia; refraction was +4.35 -0.75 × 13° OD and +9.25 -3.75 × 2° OS. Biometry showed a flat corneal radius (R1 8.76 mm, R2 8.28 mm) and axial length of 23.25 mm. We decided to implant the IC-8 and targeted a slight hyperopic refraction of 0.75 to 1.00 D due to predicted axial growth in the patient’s left eye.
At 3 months postoperative, his refraction was +4.00 -3.00 × 43° OS, and UCVA was 0.5 logMAR at distance and 0.4 logMAR at near; BCVA was 0.15 logMAR at distance, and distance-corrected near visual acuity was 0.1 logMAR. Refraction and visual acuities stayed stable for a follow-up period of 24 months.
Fundamental 5: Refractive EDOFs offer extended depth of focus without a diffractive optic design
The Lentis Comfort LS313-MF15 (Oculentis) adopts the concept of combining a refractive bifocal profile with EDOF of 1.50 D at the IOL plane, obtained through reduced add power within the lower part of this rotationally asymmetric IOL.17,18 Another lens, the Miniwell (Sifi Medtech), instead uses three symmetrical concentric zones with different amounts of spherical aberration to create a progressive multifocal zone from distance to near. These technologies are promising and show good results, but their success depends on the degree of higher-order aberrations in the cornea.
Examples of Refractive EDOFs IOLs
- Lentis Comfort LS313-MF15 (Oculentis)
- MiniWell (Sifi Medtech); progressive multifocality with three zones
- WIOL-CF (Medicem); bioanalogic haptic-less IOL
Case report. An 85-year-old patient presented with binocular cataract and a BCVA of 0.5 logMAR OD and 0.6 logMAR OS. Because the patient was a hunter, he desired minimal dysphotopic phenomena but still wanted the ability to perform the activities related to his hobby, including cleaning and loading his rifles, without the need of spectacles.
We decided to perform laser cataract surgery using the Lensar laser (Lensar) with implantation of the Femtis Laser Lens LB-313 MF15 (Oculentis) in both eyes. This lens is a modified Lentis Comfort LS-313 MF15 (Oculentis); the optical profile is the same, but haptic modification allows the IOL optic to be enclaved in a perfectly round anterior capsulotomy to offer high refractive stability.
Postoperatively, the patient’s monocular distance UCVA was -0.1 logMAR in both eyes, with a continuous intermediate visual acuity at 90, 80, and 60 cm of greater than 0.1 logMAR. Evaluation of photic phenomena using the Halo & Glare Simulator (Carl Zeiss Meditec) and the McAlinden questionnaire19 showed no side effects and high satisfaction.
1. Linz K, Attia MS, Khoramnia R, et al. Clinical evaluation of reading performance using the Salzburg Reading Desk with a refractive rotational asymmetric multifocal intraocular lens. J Refract Surg. 2016;32(8):526-532.
2. Kretz FT, Koss MJ, Auffarth GU, et al. Intermediate and near visual acuity of an aspheric, bifocal, diffractive multifocal intraocular lens with +3.25 D near addition. J Refract Surg. 2015;31(5):295-299.
3. Kretz FT, Bastelica A, Carreras H, et al. Clinical outcomes and surgeon assessment after implantation of a new diffractive multifocal toric intraocular lens. Br J Ophthalmol. 2015;99(3):405-411.
4. Kretz FT, Attia MA, Linz K, Auffarth GU. Level of binocular pseudoaccommodation in patients implanted with an apodised, diffractive and trifocal multifocal intraocular lens. Klin Monbl fur Augenheilkd. 2015;232(8):947-952.
5. Attia MS, Auffarth GU, Khoramnia R, et al. Near and intermediate reading performance of a diffractive trifocal intraocular lens using a reading desk. J Cataract Refract Surg. 2015;41(12):2707-2714.
6. Kretz FT, Gerl M, Gerl R, et al. Clinical evaluation of a new pupil independent diffractive multifocal intraocular lens with a +2.75 D near addition: a European multicentre study. Br J Ophthalmol. 2015;99(12):1655-1659.
7. Kretz FT, Breyer D, Klabe K, et al. Clinical outcomes after implantation of a trifocal toric intraocular lens. J Refract Surg. 2015;31(8):504-510.
8. Gerl M, Breyer DRH, Hagen P, et al. Clinical comparison of a trifocal and a trifocal-toric intraocular lens based on the same diffractive platform. Klin Monbl fur Augenheilkd. 2017;234(10):1276-1282.
9. Kretz FT, Choi CY, Muller M, et al. Visual outcomes, patient satisfaction and spectacle independence with a trifocal diffractive intraocular lens. Korean J Ophthalmol. 2016;30(3):180-191.
10. Kretz FT, Muller M, Gerl M, et al. Binocular function to increase visual outcome in patients implanted with a diffractive trifocal intraocular lens. BMC Ophthalmol. 2015;15:110.
11. Kretz FT, Breyer D, Diakonis VF, et al. Clinical outcomes after binocular implantation of a new trifocal diffractive intraocular lens. J Ophthalmol. 2015;2015:962891.
12. Hohn F, Tandogan T, Breyer DR, et al. Functional results one year after implantation of a bitoric, trifocal intraocular lens. Klin Monbl fur Augenheilkd. 2015;232(8):957-961.
13. Breyer DRH, Kaymak H, Ax T, et al. Multifocal intraocular lenses and extended depth of focus intraocular lenses. Asia-Pacific J Ophthalmol. 2017;6(4):339-349.
14. Attia MSA, Auffarth GU, Kretz FTA, et al. Clinical evaluation of an extended depth of focus intraocular lens with the Salzburg Reading Desk. J Refract Surg. 2017;33(10):664-669.
15. Kaymak H, Hohn F, Breyer DR, et al. Functional results 3 months after implantation of an “extended range of vision” intraocular lens. Klin Monbl fur Augenheilkd. 2016;233(8):923-927.
16. Tarib IK, Herbers C, Hagen P, et al. Postoperative results in patients implanted with a novel enhanced depth of focus intraocular lens. EC Ophthalmol. 2018;9(4):192-202.
17. Kretz FT, Khoramnia R, Attia MS, et al. Clinical evaluation of functional vision of +1.5 diopters near addition, aspheric, rotational asymmetric multifocal intraocular lens. Korean J Ophthalmol. 2016;30(5):382-389.
18. Tarib IK, Herbers C, Hagen P, et al. Benefits of a rotationally asymmetric enhanced depth of focus, Bifocal segment intraocular lens in an older cataract population ranging from 74 to 82 years. EC Ophthalmol. 2018;9(5):248-256.


