

The equipment the surgeon uses in the OR should feel like an extension of his or her hands. Not only should it be comfortable to use, it should also be reliable, stable, and capable of precise maneuvers. This is especially true for retinal surgery, where careful micromovements are needed to dissect and operate on delicate tissue, and where the surgeon often has to make critical adjustments based on the anatomy he or she encounters. Thus, there is another element that is essential to surgical confidence: the degree of control the surgeon has over the equipment and whether it is responsive and adaptable to one’s personal preferences.

Figure 1. The OS4 platform is versatile and responsive, which helps surgeons provide patients with the best possible outcomes.
I have had personal experience using several of the vitrectomy platforms available on the market. Each has its benefits and downsides. In my view, many of the technologies require the surgeon to learn a certain way of performing surgery, either because of the onboard settings or because they are limited in their functionality. I find the opposite to be true of the Oertli OS4 surgical platform (Figure 1). Not only does the OS4 come with several advanced features, it is also responsive and is capable of doing exactly what I need to provide patients the best possible outcome. Instead of having to retrain myself to use the OS4, the platform is versatile enough that I can maintain my surgical preferences while still being confident that I am performing excellent surgeries.
I have had personal experience using several of the vitrectomy platforms available on the market. Each has its benefits and downsides. In my view, many of the technologies require the surgeon to learn a certain way of performing surgery, either because of the onboard settings or because they are limited in their functionality. I find the opposite to be true of the Oertli OS4 surgical platform (Figure 1). Not only does the OS4 come with several advanced features, it is also responsive and is capable of doing exactly what I need to provide patients the best possible outcome. Instead of having to retrain myself to use the OS4, the platform is versatile enough that I can maintain my surgical preferences while still being confident that I am performing excellent surgeries.
Advanced HDC Fluidics
The OS4 is designed with several advanced features, but its most important element is its High Definition Dynamic Direct Control (HDC), which functions as a brain, monitoring and controlling all onboard functions and intuitively adjusting parameters. Yet, the interface is easy to use and user friendly, thus minimizing the time it takes to reprogram and recalibrate between OR sessions. If this feature is a brain, it is a natural extension of the surgeon’s brain, putting two “minds” to work during every case.
Perhaps the most innovative aspect of the OS4 platform is its next generation fluidics, including the ability to quickly switch between three different pump modes: peristaltic, Venturi, and SPEEPMode. Understanding the principles of pump and fluid dynamics will help explain why having these options can be beneficial.
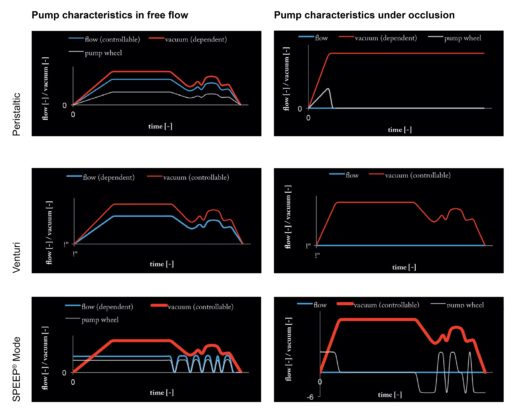
Figure 2. Pump characteristics in free flow and under occlusion.
In posterior segment surgery, the surgeon is manipulating delicate tissue in a tight space with limited visibility. When he or she is removing vitreous, the dynamics of the pump and its relationship to vacuum and aspiration are critical for safe maneuvers (Figure 2). The peristaltic pump creates a relative vacuum when the aspiration port is occluded; the operator controls flow rate with the foot pedal but cannot adjust the vacuum. In practical terms, when the tip is not occluded, the fluid level in the eye is maintained, and the vacuum engages at the lowest level required to remove the vitreous when the tip becomes occluded. Such a system may have distinct advantages at the start of surgery during the core vitrectomy, in the periphery where tractional forces are more consequential, or when dissecting near fragile vitreomacular adhesions.
With Venturi, the vacuum is controlled by pedal and the flow by preset parameters, meaning that the fluid turnover in the eye depends on the vacuum power, size of the aspiration port, and the condition of the material being aspirated. Such systems require less movement of the tip to engage and remove vitreous; however, they also attract material less discretely than peristaltic pumps, and thus, may create unwanted tractional forces.
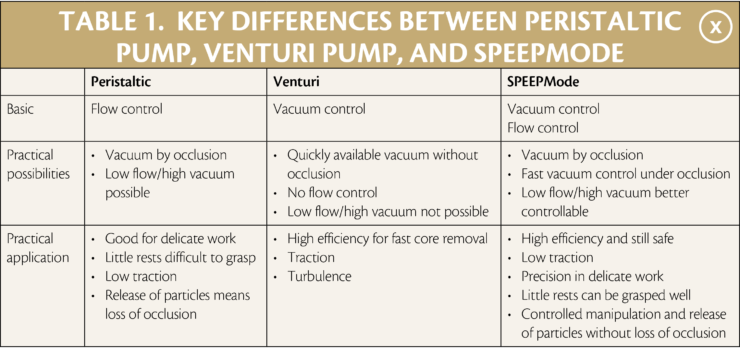
Fundamentally, with the peristaltic pump, the pedal determines flow, vacuum occurs when the tip is occluded until the preset value, and there is a possibility to work with low flow at high vacuum. With the Venturi pump, the pedal determines vacuum, flow results from vacuum and the resistance of the tubing, vacuum level remains constant when the tip is occluded, and there is no independent control of flow and vacuum. Additional differences are seen in Table 1 and Figure 3.
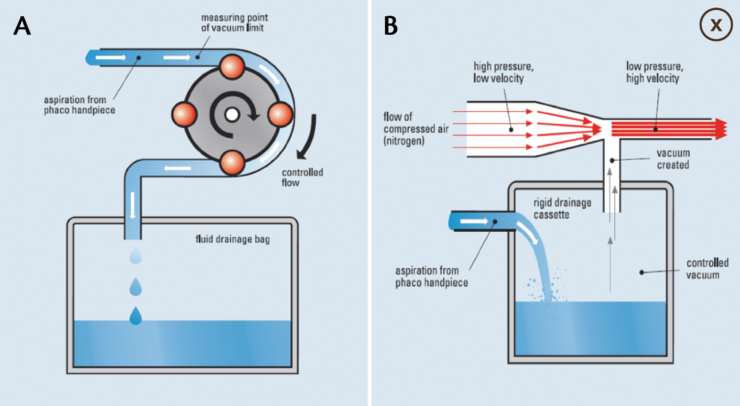
Figure 3. Peristaltic pumps (A) employ rollers to compress the tubing system to create flow while a preset vacuum level is engaged when the port is occluded. As the port becomes occluded, the rollers slow down, yielding decreased outflow. Venturi systems (B) operate on a different principle, where the flow is generated by compressed air, the air nozzle is connected to a closed drainage bag, and vacuum is constantly on.
Within the dynamics of surgery, there is not much difference when the tip is not occluded. However, tip occlusion with a peristaltic pump results in a high vacuum surge, often to uncontrollable levels. With Venturi, the surgeon gains greater control over the vacuum, but flow drops to zero when the tip is occluded.
What differentiates the OS4 platform from others is the availability of a third option, SPEEPMode, which gives surgeons access to the best features of peristaltic and Venturi. Using this mode, which offers controlled flow and vacuum, I am able to maintain the holding force of the vacuum, enabling the highest degree of efficacy while also assuring safety and control of flow. In my hands, this is the ideal setting for controlled lifting of epinucleus; aspiration of cortex, especially when zonulas are weak; creating a posterior vitreous detachment or detaching posterior hyloid; and for working precisely and controlled in the periphery with or without detached retina.
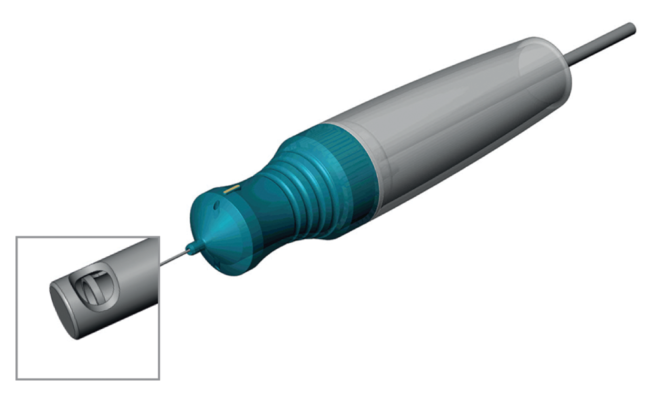
Figure 4. The Continuous Flow-Cutter has a cutting speed of up to 10,000 cuts per minute.
Continuous Flow-Cutter
The advanced flow dynamics available with the OS4 platform are important on their own, but they also complement and enhance other performance features. For example, the Continuous Flow-Cutter with cutting speeds up to 10,000 cuts per minute (Figure 4). Yet speed is only one aspect of the performance of the vitrector. In theory, a faster cut speed reduces turbulence because it is performing smaller cuts with each pass of the blade. With traditional guillotine-style vitrectors, material enters the port during the “open” phase, which is then cleaved while the blade action moves to the “closed” position. At faster speeds, less material is cleaved with each blade action compared with slower speeds, which should mean less repulsion of vitreous in the periods when the blade is fully closed.
Videos. Standard guillotine-style cutter versus Continuous Flow-Cutter.
However, even at very high cut rates, the closed action of a guillotine cutter results in an intermittent disruption of flow. This results in a wavelike action in the material being cut—in this case, the vitreous—as a result of the stop and start of flow during open and closed blade action phases (Figure 5). There may be minimal to no consequence for this loss of holding force when operating in most parts of the retina; over delicate tissue and especially in the peripheral regions, it may be a different story. The OS4 changes this by allowing the surgeon the ability to use continuous flow, meaning that cutter port is constantly open. With a classic guillotine cutter, the port is open only half of the action time, resulting in interruption of flow and consequential loss of vacuum and holding force at the tip. With the Continuous Flow-Cutter, the port is continuously open almost 100% of the time, meaning continuous flow and no loss of vacuum or holding force at the tip.
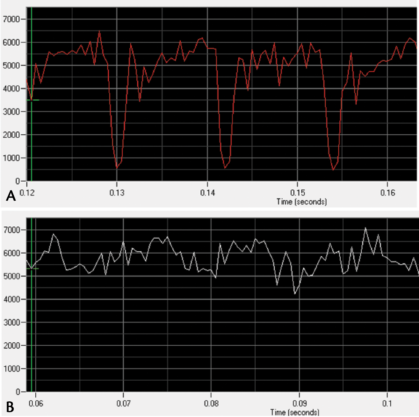
Figure 5. Graphs depicting flow rates in traditional guillotine-style cutters (A) and the Continuous Flow-Cutter with the OS4 platform (B). Whereas the flow is intermittently interrupted by the closed action of the blade in graph A (identified as zeroing of the flow), the flow is relatively stable in graph B.
Personal Experience
I prefer to use 25-gauge instrumentation for most of my surgeries, and in my hands, I find the Oertli OS4 system to be absolutely reliable and stable. It provides an unprecedented level of precision, control, and responsiveness to adjustments to the foot pedal. Overall, since bringing this technology into my OR, I have gained more confidence while performing more efficient surgeries with reduced vitrectomy time.
More recently, I have had the opportunity to try 27-gauge surgery with this platform and I was pleasantly surprised with the stiffness of the instruments. I would have expected more flexibility, especially as I maneuvered out to the periphery. Instead, the instruments maintained their shape and did not bend or become lax. While the vitreous removal was understandably slower compared with larger gauge systems, it was still very efficient and the constant flow contributed to better performance.
Conclusion
The OS4 has several features that contribute to “quiet” surgeries where the vitreous and retina are only minimally disrupted. It is a stable and reliable platform that is supported by well-designed and manufactured instrumentation that provide the surgeon with the tools necessary for careful manipulation of delicate tissue of the retina, macula, and vitreous. These features are evident in other integrated functionalities. For example, the OS4 can automatically maintain the IOP within the globe during a gas or oil fill when this step is done under air, resulting in added safety and reliability.
All of these things are very useful features and they add up to make the OS4 a high-technology, versatile surgical platform for use in every kind of posterior segment surgery. What I find most impressive about the system, however, is that it seems to adapt to the way I want to perform surgery, and I have not had to compromise the way I want to perform because of the settings of the machine.