
The usefulness of the femtosecond laser in certain steps of the cataract surgery procedure is well established. Some advocate for its use in all cases, while others reserve the femtosecond laser for certain situations or cataract types. In my OR, I use laser cataract surgery in a variety of cases, from routine to challenging. The reason that I rely on the femtosecond laser so often is simple: It is a reliable adjunct technology that helps me to achieve safe, successful cataract surgery in a timely and efficient manner.
For close to 3 years now, I have been using the Femto LDV Z8 (Ziemer) for laser cataract surgery (Figure 1). I use the laser in the following capacities: corneal incisions, capsulotomy, and nuclear fragmentation. In this article, I will discuss how I manage complex cataracts with the Femto LDV Z8.
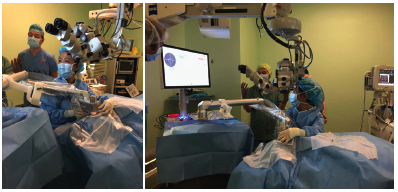
Figure 1. Professor Chee performs laser cataract surgery with the Femto LDV Z8.
I am especially impressed with the way that the Femto LDV Z8 softens the lens prior to phacoemulsification. For brunescent cataracts, I favor the 16-segment fragmentation pattern, which cuts the nucleus into finer fragments in the core and into larger segments in the less dense periphery. The nuclear fragmentation cuts are clean and deep.
I impale the nucleus deeply and then plunge my chopper into the nucleus to laterally separate the fragments. No matter where I place my chopper within the nucleus, the pieces will just fall apart because of the close spacing and radial orientation of the fracture lines. Direct chopping of the nucleus is facilitated and troughing of the nucleus is redundant, minimizing the ultrasound energy used.
HARD VS SOFT
For most surgeons, the technique for handling a dense posterior polar cataract is different from the technique used for a soft one. While the soft posterior polar cataract is manageable using conventional techniques, managing the dense posterior polar cataract is much feared because of the increased risk of posterior capsule tear and dropped nucleus, especially if the opacity is a large one.
Soft posterior polar cataract. In the nonlaser management of a soft posterior polar cataract, the surgeon uses hydrodelineation to cleave the nucleus into the endonucleus and an epinuclear shell. Dealing with the endonucleus is easy, but the epinuclear cortex created by the fluid wave is often thick and sticky. Its removal can be challenging, and it often takes longer dealing with than removing the endonucleus. This is partly because the thickness of the epinuclear shell—created by hydrodelination—is not precise and one errs on the side of caution, resulting in the epinuclear plate being thicker than necessary to avoid entering the plane of the polar opacity and posterior capsule rupture.
With the Femto LDV Z8, surgery is converted into an effective and safe procedure. I do not increase the posterior capsule offset for nuclear fragmentation, which is kept to the minimum of 600 µm. Safety is created because I can easily remove the fragmented nuclear pieces without the need to rotate the epinucleus delineated by the laser. This acts as a cushion, maintaining the integrity of the posterior capsule. The laser fragmentation also aids in reducing the ultrasound energy.
Furthermore, I avoid hydrodissection and hydrodelamination. Instead, I perform subcapsular viscodissection in the subincisional sites to release the epinucleus up to the lens equator, as this portion of the epinucleus can be extremely sticky. This is done after ensuring that the capsulotomy is complete and before inserting the phaco probe. Finally, with the femtosecond laser, I am assured of achieving a circular 5-mm capsulotomy that is perfectly centered and can be used for optic capture in the event of significant posterior capsule compromise.
With this technique, I have reduced my rate of posterior capsule rupture in soft posterior polar cataracts to approximately 3%.
Hard posterior polar cataract. When dealing with a hard posterior polar cataract, I avoid hydrodelineation completely and do viscodissection, as in the soft posterior polar cataract technique. I use the minimum posterior capsule offset of 600 µm for nuclear fragmentation and maintain a 5-mm capsulotomy. I prefer the 16-segment fragmentation pattern.
I modify my technique by first creating a central deep groove to create space. I crack the nucleus at both ends of the trough and avoid using cracking maneuvers in the center. The heminucleus, located away from the sideport, is cracked in half by keeping the phaco needle deep within the trough, providing counterforce as the long chopper, such as a Nagahara chopper, performs a horizontal chop along the laser fragmentation plane. The other heminucleus is impaled distally with the phaco needle bevel side down, and the nucleus is separated in half along the laser cut plane using the chopper.
The distal quadrants are first emulsified and removed without nuclear rotation. Subsequently, the proximal quadrants are emulsified, removing the quadrant lying between the two incisions last. The posterior capsule may dehisce at this stage if the nucleus is adherent to the polar opacity; however, I have never encountered a dropped nucleus while the fragment is safely being emulsified and removed. As the nucleus is removed without the need to rotate the cataract, the integrity of the posterior capsule is preserved during nuclear removal.
The epinucleus is typically very thin in dense posterior polar cataracts—because of the 600 µm posterior capsule offset—meaning that it is not thick and sticky. When using viscodissection in combination with the Femto LDV Z8, performing cataract surgery on a posterior polar cataract is almost like a routine case. On one day in particular, I performed laser cataract surgery on seven posterior polar cataracts consecutively. One of my colleagues remarked, “You know, this is like a routine cataract for you. The speed at which you do it is like it’s routine.”
KNOW YOUR SYSTEM
The key to achieving consistently excellent results with laser cataract surgery is to understand the system that you are using inside and out as well as how to use it during each key step of the procedure. With the Femto LDV Z8, this could not be easier.
The system. The high-frequency laser oscillator of the Femto LDV is robust to environmental factors including temperature and humidity or physical movements; the Femto LDV can be moved and rolled around. It is also the only femtosecond laser available today to use low energy—in the nanojoule range—with high repetition rate—in the megahertz range—to achieve highly precise results with minimal side effects.1,2
Docking. The Femto LDV Z8 uses a fluid-filled patient interface, and this feature reduces the increase in IOP that is typical during the docking stage with all femtosecond laser systems. However, with a liquid interface, the IOP increase is less than with a curved interface.3 Another advantage of the fluid-filled interface is that it also eliminates the risk for corneal folds, which can lead to incomplete capsulotomies.3 (For more information on low-pulse energy, see The Advantages of a Low-Energy Laser.)
THE ADVANTAGES OF A LOW-ENERGY LASER
Low pulse energy is an important factor in laser cataract surgery. The Femto LDV Z8 (Ziemer) produces a very small focus by using high-repetition, low-energy overlapping pulses (Figure 1). This enables a smooth cut,1 which is easy to open and free from tissue bridges,2 and a shorter procedural time. The Femto LDV Z8 works with a handpiece that is docked to the interface and fixed by vacuum on the patient’s eye. Since the laser optic is integrated into the handpiece, its very short distance to the eye allows creation of miniscule laser spots to separate the tissue. Thus, only little energy is needed.
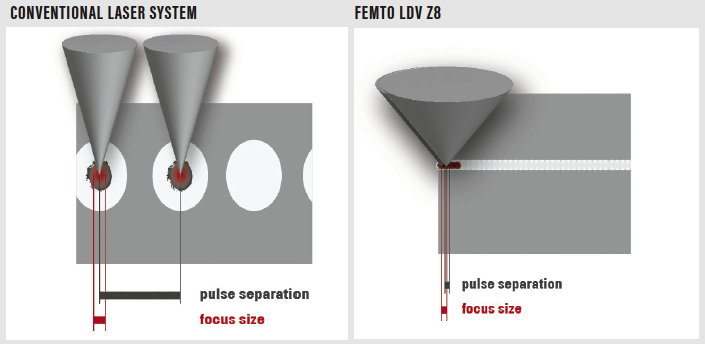
Figure 1. The spot size of conventional femtosecond laser systems (left) versus the Femto LDV laser (right).
1. Williams GP, George BL, Wong YR, et al. The effects of a low-energy, high-frequency liquid optic interface femtosecond laser system on lens capsulotomy. Nature. 2016;6:24352. doi: 10.1038/srep24352.
2. Lubatschowski H. Applications of the femtosecond laser. Cataract & Refractive Surgery Today Europe. 2012.
With the Femto LDV, docking is always achieved perpendicularly, even in the event that the patient’s head is tilted. This is because the handpiece of the laser allows the patient interface to be docked according to surgeon preference; this differs from other systems, which require the surgeon to lower the head of the laser to the patient. In that scenario, the patient’s head must be free of any tilt in order to achieve proper docking.
The first step to achieving a proper dock with the Femto LDV Z8 is to place the suction ring well centered on the patient’s eye. Thereafter, suction is applied as the patient interface is filled with balanced saline solution. The interface is free from bubbles, so that it does not block the laser treatment.
One tip for the beginning surgeon is that, when initiating the dock, look through the viewing window on top of the laser handpiece. This will provide a clear view to the eye. Docking can then be completed perfectly once the eye is centered in this viewing hole.
Capsulotomy. Achieving a perfect dock simultaneously to the laser approaching the capsule is extremely crucial, especially when treating an intumescent cataract. This is so that the capsule does not become perforated asymmetrically and, thus, the lens does not decompress and egress too rapidly, causing an uncontrolled extension of the laser capsulotomy. When this maneuver is done correctly, an intact and safe capsulotomy is achieved.
In the event that the capsulotomy appears to be incomplete—which is rare in my experience—I stain the capsule with trypan blue dye to identify the tags or bridges. In most cases, the cause of the incomplete capsulotomy is micro-adhesions, which can simply be pulled radially to safely achieve a complete and strong capsulotomy.
CONCLUSION
I have used the Femto LDV Z8 femtosecond laser for many types and for many grades of cataracts. Whether the cataract is hard or soft, there are many advantages to performing laser cataract surgery. Specifically with the Femto LDV Z8, I have seen great benefit in adding this technology in my OR. I appreciate the ease with which the patient interface docks as well as the complete capsulotomies it can safely create in any case, even for the patient with an abnormal posture when supine. This technology will continue to be a mainstay for me and for my practice.
1. Lubatschowski H. Applications of the femtosecond laser. Cataract & Refractive Surgery Today Europe. 2012.
2. Riau AK, Liu Y-C, Lwin NC, et al. Comparative study of nJ- and mJ energy level femtosecond lasers: evaluation of flap adhesion strength, stromal bed quality, and tissue responses. Invest Ophthalmol Vis Sci. 2014;55:3186–3194. DOI:10.1167/iovs.14-14434.
3. Talamo et al. Optical patient interface in femtosecond laser–assisted cataract surgery: Contact corneal applanation versus liquid immersion. J Cataract Refract Surg. 2013;39:501-510.



