
Technological advances in cataract surgery have greatly improved postoperative visual results. In return, patient expectations and demands in terms of their optical and refractive effects have increased. The use of the femtosecond laser in cataract surgery has been a great step forward in providing safety and reproducibility in the critical stages of cataract surgery, such as the capsulorrhexis and nucleus fragmentation. The FEMTIS IOL (Oculentis) takes advantage of the perfectly circular capsulorrhexis made by the femtosecond laser to anchor the IOL with specially designed haptics. As a result, the lens has greater stability and centration in the long-term.
In this preliminary phase of the lens’ development, the FEMTIS is only available as a monofocal lens; however, it is expected to be very useful as a toric and multifocal platform in the near future, since these could be the designs that benefit the most from this novel idea.
In traditional lens implantation, the IOL is kept in place in the capsular bag by the back-pressure of the capsule against the haptics. Capsular shrinkage and fibrosis increase the pressure on the haptics, which can lead to decentration, tilt, and rotation of the lens and can result in induced higher-order aberrations (HOAs) and decreased optical quality of the visual system.
We recently investigated the tilt of the FEMTIS IOL, and these results are part of an international multicentered study led by Gerd U. Auffarth, MD, PhD, from the International Vision Correction and Research Centre and the David J. Apple Laboratory, University of Heidelberg, Department of Ophthalmology.
WHAT WE KNOW ABOUT IOL TILT
According to theoretical reports, coma increases with rising IOL tilt and decentration.1,2 The impact of this misalignment depends on IOL design, and aberration-correcting IOLs seem to be very sensitive to decentration and tilt.3 On the other hand, tilt angle has statically significant effects on the HOA profile using a physical eye model and traditional IOL inserted in capsular bag. In this last report,3 the mean tilt was 5.7º. Further, Peng et al found that the IOL tilt in horizontal and vertical directions in eyes in which a manual capsulorrhexis was created was significantly higher than those in which a laser capsulotomy was created, with a mean tilt over 2.3°.4
On average, a 2º to 3º tilt is common. More than a 10º tilt and above 1 mm decentration are occasionally reported with modern cataract surgery (about 10% of the pseudophakic population).5 Mester et al compared the tilt and decentration of a one-piece aspheric IOL and the position of the natural crystalline lens in young individuals. As a result, all lenses were tilted upward (mean 2.2º, crystalline lens; 2.5º, IOL) and to the temporal side (mean 3.1º, crystalline lens; 2.6º, IOL).6 Another report showed a mean optic tilt of 2.89º ±1.46 standard deviation (SD) for the spherical IOL and 2.85º ±1.36 SD for the aspheric IOL.7 This finding indicates that a significant relationship is found between aspheric IOL tilt and internal coma aberration and suggests that the tilt of aspherical IOLs should be reduced as much as possible.8
ASSESSMENT OF FEMTIS IOL TILT
The FEMTIS IOL is a foldable hydrophilic acrylic lens (its material is known as Hydrosmart), with a biconvex aspheric optic with a continuous 360° barrier edge; the lens has marks on the front surface to aid in measuring rotation. The lens haptics have a clip design with barrier edge, with two longitudinal flaps and two small lateral flaps to hold the rhexis (Figure 1).
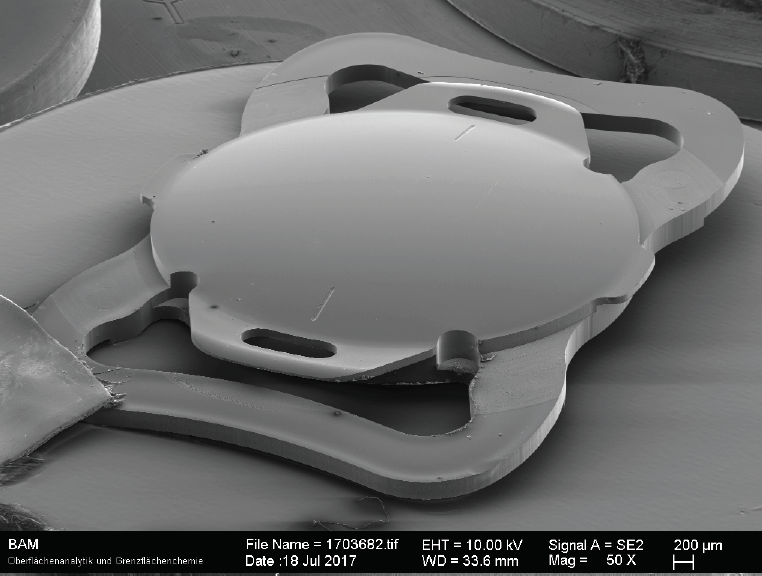
Figure 1. Image of the FEMTIS IOL taken by reflection electron microscope.
In the study, we implanted the FEMTIS IOL bilaterally in 25 patients, after a 4.8-mm capsulorrhexis was performed with the Lensar Laser System. In all cases, the capsulorrhexis was centered on the pupil. However, with this laser it is also possible to center the capsulorrhexis other references, such as the central axis of the lens, the visual axis, and, in special cases, kappa or alpha angle variations. Limbal markings at 0° and 180° were made preoperatively with the patient sitting upright and focusing on a distant target.
Measurement of lens position was performed at mydriasis with Pentacam Scheimpflug 2-D imaging before surgery and at 6 to 8 weeks and 6 months postoperatively. To achieve this, we drew a blue line on the Pentacam image to represent the plane of iridocorneal angle and a red line to represent the plane of visible crystalline lens (preoperative) or the implanted FEMTIS (postoperative). The angle γ between both is the lens position, which was evaluated both horizontally and vertically. Tilt (movement) was evaluated by calculating the differences between the pre- and postoperative lens positions (Figure 2).
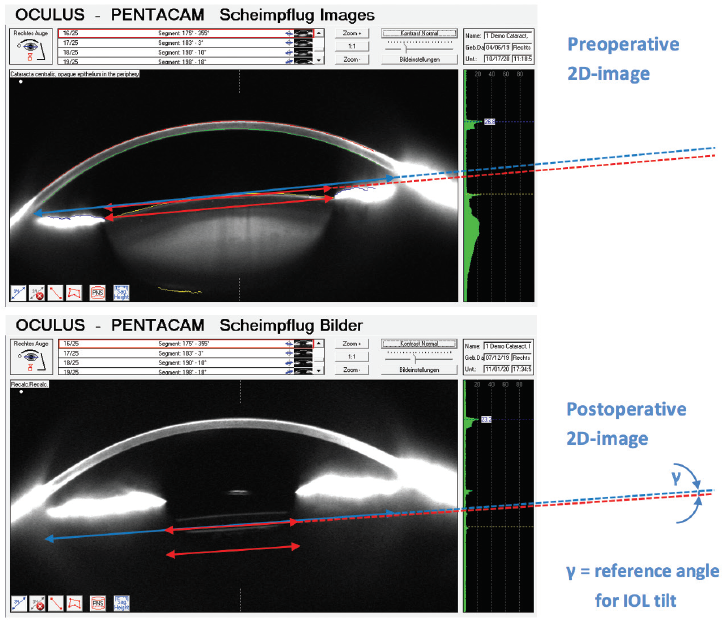
Figure 2. Method to assess IOL tilt.
PROMISING OUTCOMES
A total of 25 patients (average age, 75 years; range, 63–87 years) were included in the study. Preoperatively, the mean position of the crystalline lens was 0.04º horizontal and -0.17º vertical, which represents the natural angulation of capsular bag. Six to 8 weeks after cataract surgery and FEMTIS IOL implantation, the mean IOL position was -0.04º horizontal and -0.09º vertical. The most significant variable in this assessment was the average difference between preoperative and 6- to 8-week postoperative lens position showing the absolute value of tilt movement, which was quite low: 0.73º horizontal and 1.04º vertical (Table 1).
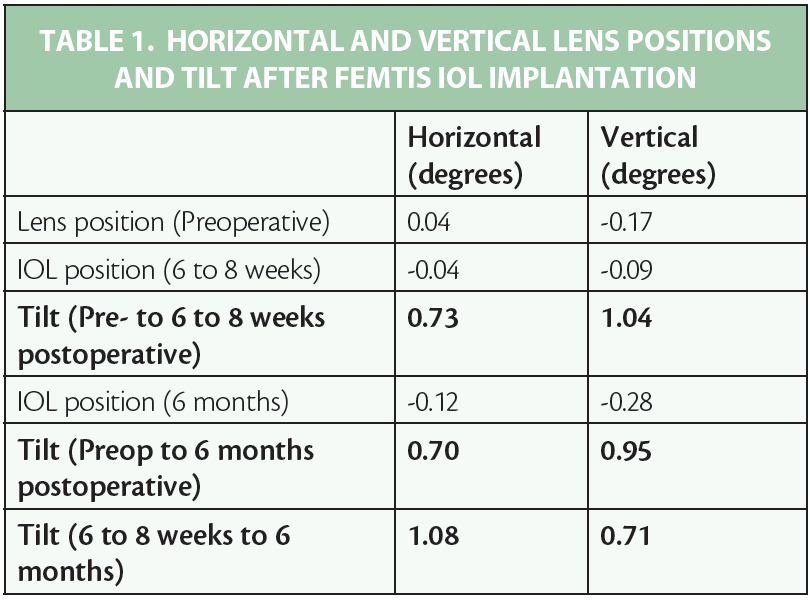
Six months after implantation, the mean IOL position was -0.12º horizontal and -0.28º vertical. The average tilt movement between preoperative and 6-month postoperative was 0.70º horizontal and 0.95º vertical. Finally, the mean tilt movement between 6 to 8 weeks postoperative and 6 months postoperative was 1.08º horizontal and 0.71º vertical. These results are, to date, much lower than those reported in the revised publications.
Optical and refractive variables were also promising. On average, from a preoperative UDVA of 0.56 logMAR (corrected 0.34), the group of patients implanted with the FEMTIS IOL achieved an UDVA of 0.15 logMAR within the first 7 days postop, 0.08 logMAR at 6 to 8 weeks, and 0.15 logMAR at 6 months. The mean preoperative spherical equivalent of refraction was 0.74 D, and then 0.09 D at 6 to 8 weeks postoperative and 0.16 D at 6 months.
From this study, we determined that the tilt evaluated with the FEMTIS IOL is quite low compared with the position of the lens preoperatively, and is also stable up to the preliminary follow-up of 6 months.
CONCLUSION
We are currently expanding our experience with FEMTIS IOL implantation and extending follow- to assess long-term stability. While emerging designs of new IOLs offer improved quality of vision and therefore better quality of life, the optimum performance is widely affected by the position of the implanted IOL in the eye.
The FEMTIS system of hooking into the capsulorrhexis is a breakthrough that must be studied in the long-term as an option to enhance the predictability and stability of the IOLs. It is also possible that, in the future, this design could be used for toric and multifocal IOLs.
1. Eppig T, Scholz K, Löffler A, et al. Effect of decentration and tilt on the image quality of aspheric intraocular lens designs in a model eye. J Cataract Refract Surg. 2009;35:1091-1100.
2. Pieh S, Fiala W, Malz A, Stork W. In vitro strehl ratios with spherical, aberration-free, average, and customized spherical aberration-correcting intraocular lenses. Invest Ophthalmol Vis Sci. 2009;50:1264-1270.
3. McKelvie J, McArdle B, McGhee C. The influence of tilt, decentration, and pupil size on the higher-order aberration profile of aspheric intraocular lenses. Ophthalmology. 2011;118(9):1724-1731.
4. Peng TT, Wang Y, Bao XY. Preliminary report on the application of femtosecond laser-assisted anterior capsulotomy in intumescent white cataract surgery. Zhonghua Yan Ke Za Zhi. 2017;53(4):281-287.
5. Ale JB. Intraocular lens tilt and decentration: a concern for contemporary IOL designs. Nepal J Ophthalmol. 2011;3(1):68-77.
6. Mester U, Sauer T, Kaymak H. Decentration and tilt of a single-piece aspheric intraocular lens compared with the lens position in young phakic eye. J Cataract Refract Surg. 2009;35(3):485-490.
7. Baumeister M, Bühren J, Kohnen T. Tilt and decentration of spherical and aspheric intraocular lenses: Effect on higher-order aberrations. J Cataract Refract Surg. 2009;35(6):1006-1012.
8. Choi SK, Kim JH, Lee D, Park SH, Maeda N, Ma KJ. IOL Tilt and Decentration. Ophthalmology. 2010;117(9):1862, 1862.e1-4.