


We often hear cataract surgeons talk about selecting the right patient for an IOL. We, however, advocate selecting the right IOL for the patient. Not only can this approach reduce the number of IOLs that must be stocked in the OR, but it can also increase patient satisfaction. This article presents four tips for deciding what IOLs you should be using in your practice.
NO. 1: USE MONOFOCAL IOLS STRATEGICALLY
It is worth considering a standard aspheric monofocal IOL whenever the following complexities are encountered:
- Difficult IOL power calculations;
- Highly aberrated corneas;
- Irregular astigmatism;
- Chronic pathology such as glaucoma, age-related macular degeneration, and uveitis;
- Mental health diagnosis; and
- Refractive error beyond the power range of currently available multifocal IOLs.
A monofocal IOL is likely to provide the most predictable outcome in these situations, but most patients will require some amount of spectacle correction after surgery.
NO. 2: TAKE FORGIVENESS INTO ACCOUNT
Whether referred to as extended depth of focus (EDOF), advanced monofocal, monofocal+, or enhanced monofocal, this new class of monofocal IOLs offers a significant advantage over premium IOLs—a larger landing zone. Such monofocal IOLs tend to be more forgiving when the IOL power calculation is slightly off target, and patients generally achieve a good visual outcome (Figure 1).
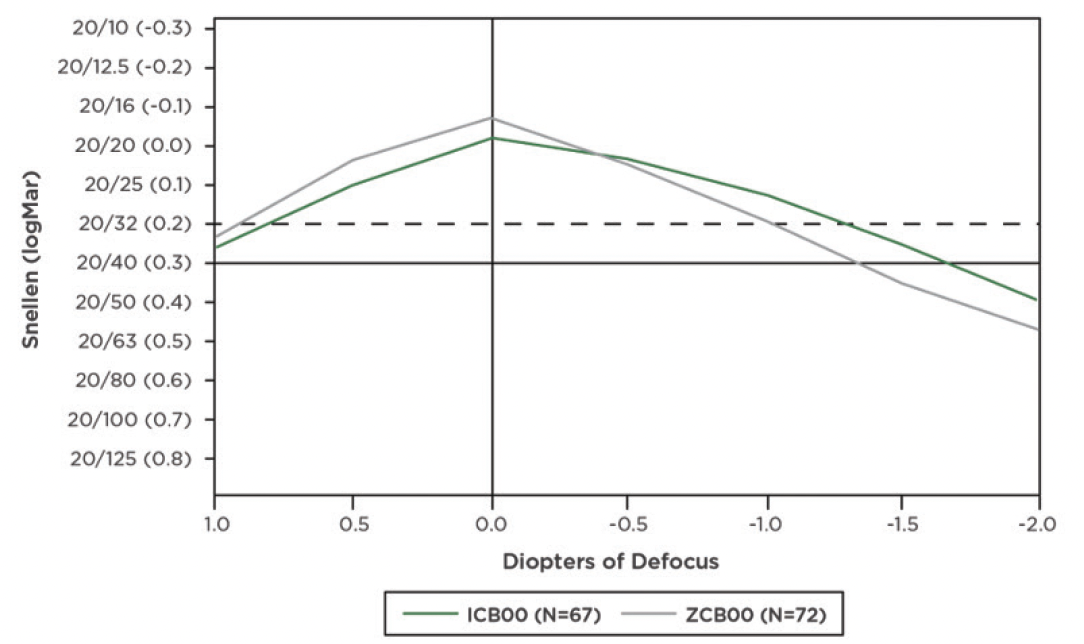
Figure 1. Defocus curves comparing an advanced monofocal IOL (Tecnis Eyhance, model ICB00, Johnson & Johnson Vision) with an aspheric monofocal IOL (Tecnis Monofocal 1-Piece, model ZCB00, Johnson & Johnson Vision).
Another benefit of this new class of monofocal IOLs is their utility in patients with complicated (eg, highly aberrated or irregular) corneas such as those with keratoconus or a history of radial keratotomy or LASIK. Toric monofocal IOLs with an extended depth of focus design can be particularly beneficial in this situation because their optical profile can reduce the risk of postoperative dysphotopsia.
Newer monofocal IOL designs can also be a good option when the following complexities are encountered:
- Difficult IOL power calculations;
- Chronic pathology such as glaucoma, age-related macular degeneration, and uveitis;
- Mental health diagnosis; and
- Refractive error beyond the power range of currently available IOLs.
Further, they can be used similarly to standard monofocal lenses with a refractive target of emmetropia. The former can also work well for a mini-monovision or monovision strategy.
NO. 3: EXPLORE PATIENTS’ VISUAL NEEDS
It is worth taking the time to understand how your patients use their vision. How highly do they value spectacle independence? Which distances are relevant to them? Do they work in an office environment? Do they drive at night often? Do they have high-contrast demands? Can they commit to compromises?
The Vivior Monitor (Vivior) is designed to provide objective evidence on how patients use their vision (Figure 2). In our experience, patients often spend more of their day using distance vision or a mix of near, intermediate, and distance vision than they realize. A Vivior assessment can facilitate the selection of an IOL that most closely matches a patient’s visual needs with a high degree of certainty because the software provides defocus curves for different IOL options (Figure 3).
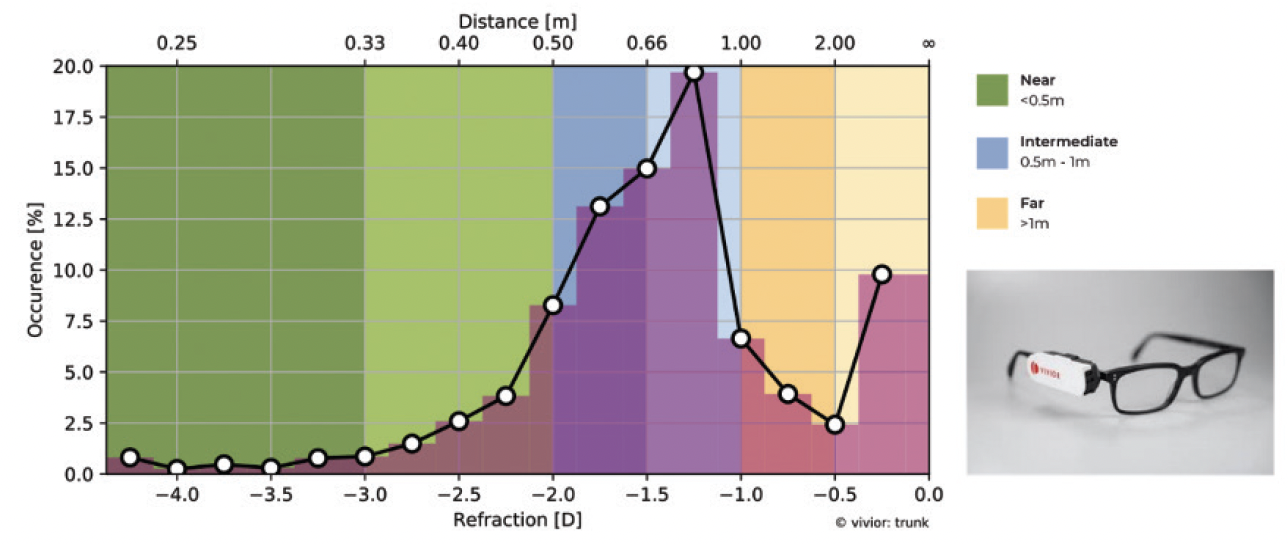
Figure 2. The defocus curve produced by the Vivior Monitor depicts where the patient utilizes their vision over the course of the day (shades of purple).
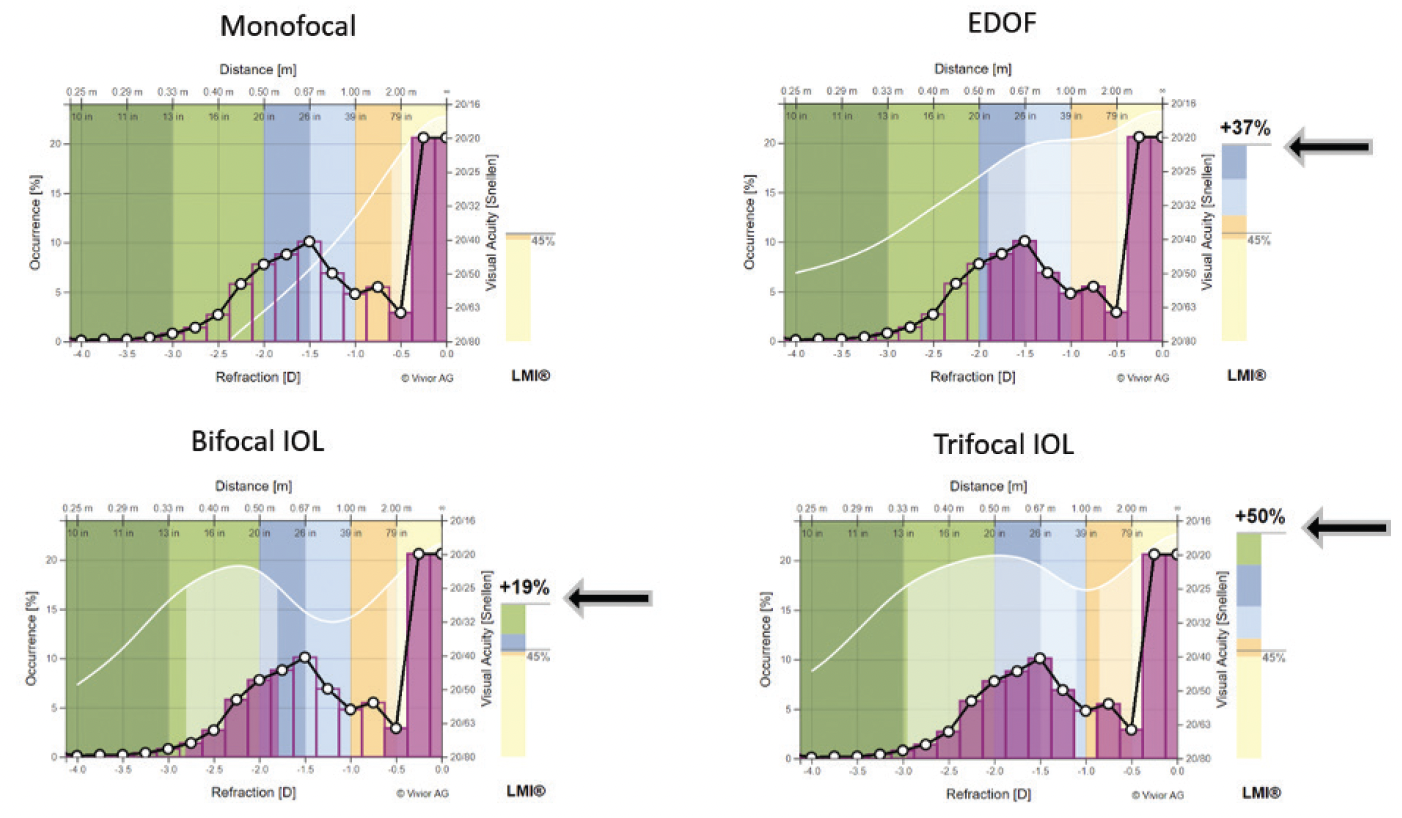
Figure 3. The Vivior software is able to apply the patient’s use of their vision (shades of purple) and estimate how different types of IOLs would meet their visual requirements.
NO. 4: CONSIDER The OPTICAL PHYSICS of the IOL
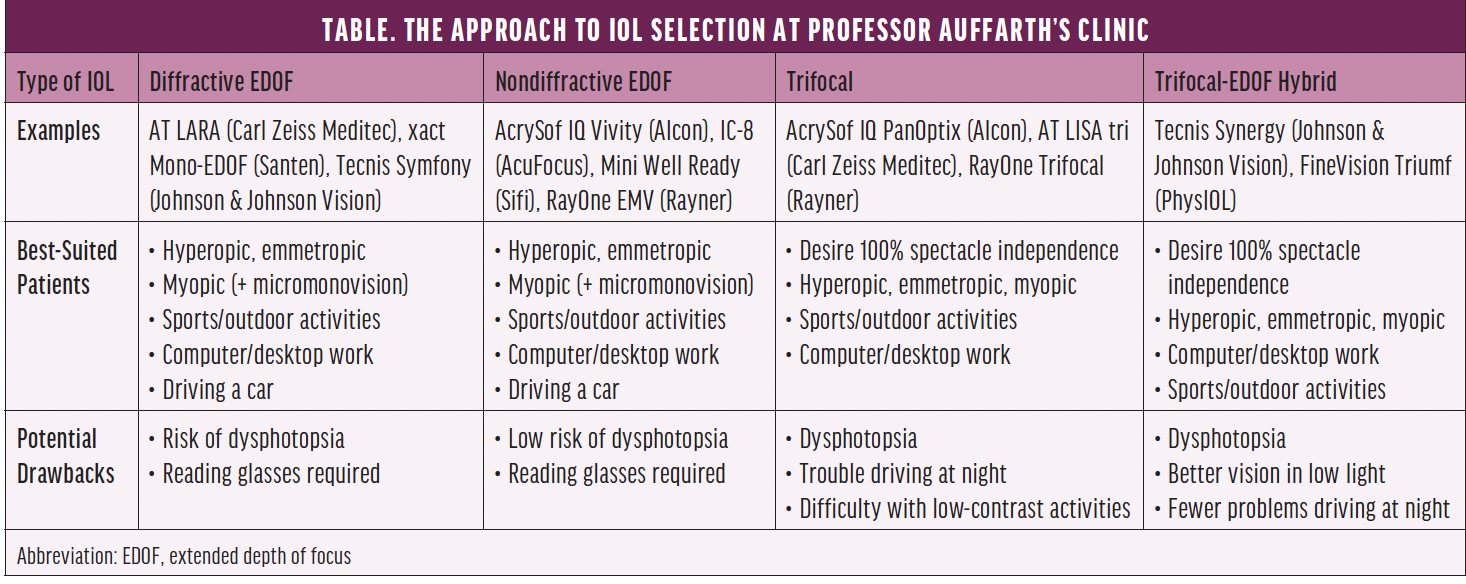
Newton’s third law of motion states that, for every action, there is an equal and opposite reaction. In keeping with this law, increasing depth of field reduces vision quality; depth of field and dysphotopsia are directly related. In other words, there are trade-offs that must be considered during IOL selection. The Table presents how one of us (G.U.A.) approaches this balancing act.
CONCLUSION
Ophthalmologists have been dreaming for more than 30 years of injectable, fluid IOLs that fill the capsular bag and mimic the natural lens. This elegant solution has not yet been achieved. With the right strategy, however, surgeons can reduce the number of IOLs required and offer patients the best possible fit for their needs.