



IOL dislocation or decentration is an uncommon complication after cataract surgery, but it can be visually troubling for the patient who experiences it. Malpositioning of the lens can cause decreases in visual acuity and can induce optical side effects such as glare and halos.
The most common reasons for early IOL dislocation are intraoperative complications such as tears in the zonular fibers, posterior capsular rupture, vitreous prolapse to the incision, residual lens cortex left in the capsular bag, and intraoperative damage to the IOL haptics, to name several. The best way to avoid early dislocation is to use good surgical technique, including creation of a continuous curvilinear capsulorhexis that covers the IOL edge and ensures capsular bag fixation of the lens.
The most common reason for late dislocation, months and even years after surgery, is pseudoexfoliation causing shrinkage of the capsular bag. Not only severe trauma but also mild trauma caused by aggressive eye rubbing or restless sleep, which can weaken the zonules, is another reason for late dislocation.
Explantation and replacement of the dislocated lens is always connected with potential risks, including loss of the capsular bag, vitreous prolapse, postoperative inflammation, and so forth. Therefore, surgical intervention must be considered carefully. This article briefly outlines my approaches to dealing with dislocated IOLs.
MINIMAL INTERVENTION
If the patient’s visual acuity is about 0.5 (Snellen decimal) and his or her age is advanced but there are no complaints of poor visual acuity or optical phenomena as a result of the malpositioned IOL, the surgical risk and the effort connected with follow-up care must be considered. In these cases, it is often best to observe the malpositioned lens and perform surgical correction only in case of worsening of the lens position or complaint from the patient.
If surgery is warranted due to visual complaints, I always proceed carefully. I try to save the existing lens if possible, thereby avoiding explantation and the implantation of a new one. For example, if a three-piece lens has been decentered, it can be stitched to the iris on one or both sides or enclaved.
If the capsular bag is dislocated in one direction, it is possible to consider implantation of a capsular tension ring (Type 9L Capsular Segment for Scleral Fixation, Morcher), affixing the ring through a scleral or Hoffmann pocket. Sometimes this maneuver does not produce a satisfactory result, however, in which case the lens must be explanted.
EXPLANTATION
When explantation is needed, I make sure to have certain tools on hand, including de Wecker angled scissors, a highly cohesive OVD such as Healon GV (sodium hyaluronate, Johnson & Johnson Vision), an anterior vitrectomy system, and triamcinolone acetonide. After creating a 2.8-mm perilimbal incision, I use the hydrodissection cannula and apply OVD under the lens to try to open the capsular bag and maneuver the lens into the anterior chamber. I then cut the lens with the de Wecker scissors into two pieces and explant the pieces separately. Alternatively, I may cut through the lens partially and turn the lens during explantation (Figure and bit.ly/rau1018). It is a very gentle and elegant technique that works best in my hands—I have tried various instruments from different companies, but they were too large and complicated.
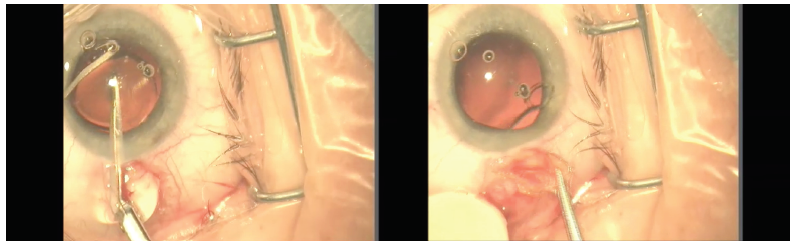
Figure. To remove this multifocal IOL, which was malpositioned due to detached haptics, Dr. Rau used de Wecker scissors to partially cut through the IOL (left) and then rotated the lens to explant it (right).
In the case of a late dislocation, if Nd:YAG laser capsulotomy has already been performed, there is usually some vitreous prolapse. This must be addressed with anterior vitrectomy, after which I stain with triamcinolone to ensure that no vitreous fibers remain in the wound.
In my opinion, it is possible to open the capsular bag only in the first 1 to 2 months after the initial cataract surgery. If reopening is possible and there is any shrinking of the capsular bag after the lens is removed, I then implant a CTR and an IOL with C-loop haptics. I avoid plate-haptic IOLs because they apply stress on the zonular fibers only in one axis, whereas the C-loop haptics distribute the stress more broadly.
If the anterior capsule is still intact, a three-piece lens can be implanted in the ciliary sulcus. If not, an Artisan Aphakia iris-fixated IOL (Ophtec) can be enclaved in an anterior, retropupillary position. If it is my opinion that the decentration of the original lens occurred due to trauma or the patient’s consistent eye rubbing, I avoid retropupillary Artisan implantation.
Sometimes, in eyes with large pupils, I use one of the Morcher IOLs with large haptics designed for scleral fixation (Type 90L, 66, or 81B), implanted though a corneoscleral incision. I prefer to use three-piece IOLs, which I stitch to the iris; however, enclavation can be considered. I regret that, at the moment, no company produces a three-piece multifocal IOL for this purpose, and I hope that production of these lenses will start again.
CONCLUSION
IOL dislocation after cataract surgery is uncommon, but surgeons must be prepared to address it when it is visually disturbing to the patient. If observation is possible, especially in elderly patients, this may be the best approach to management. For younger patients—or when visual symptoms are bothersome or debilitating to the patient—one of the surgical approaches outlined above may be helpful in resolving the situation to the satisfaction of all involved.