

As a relatively new surgeon to this space, it can be tricky to navigate the nuances of available procedures as well as patient selection. I have been performing MIGS for about 6 years. I prefer ab interno techniques like the OMNI Surgical System (Sight Sciences) as a first line surgical treatment because they are effective and have a lower risk profile.
The OMNI Surgical System is the only device combining two accepted and well-established mechanisms to alleviate outflow resistance in the conventional outflow pathway: canaloplasty and trabeculotomy (Figure 1). It also enables surgeons to treat 360º of Schlemm’s canal and address the three sources of outflow resistance (trabecular meshwork, Schlemm’s canal, and collector channels) in a single surgery via canaloplasty and trabeculotomy.
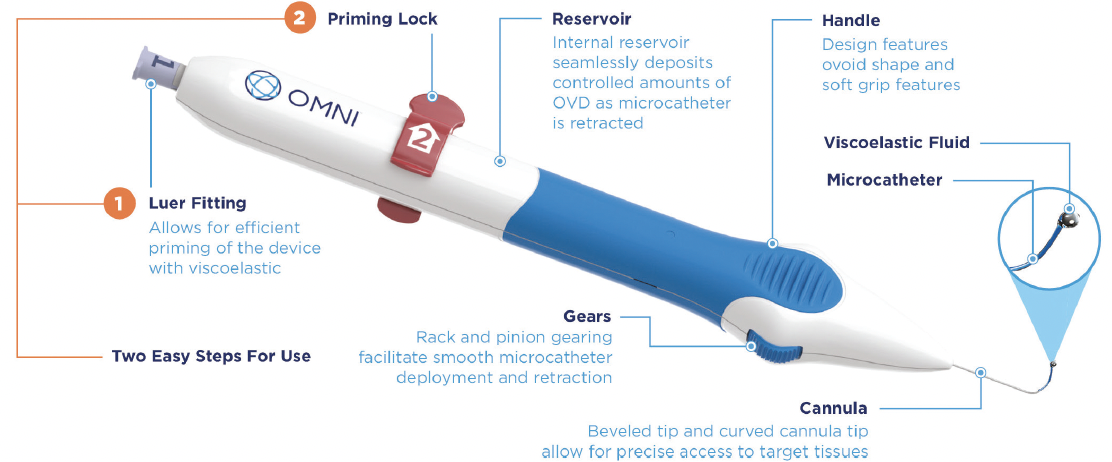
Figure 1. OMNI diagram.
Another enticing element of the OMNI procedure is its versatility as a procedure whereby canaloplasty can be performed on its own or in combination with trabeculotomy. It can also be performed in combination with cataract surgery or as a standalone procedure.
The learning curve with OMNI was short, and it took approximately 10 cases to feel confident in my surgical technique. The handheld instrument includes a cannula, microcatheter that can be used for viscodilation or tissue cutting, internal reservoir of viscoelastic, and a finger wheel. The finger wheel on the handle of the device is used to advance the microcatheter into the Schlemm’s canal to dilate it, and viscoelastic is dispensed upon withdrawal of the microcatheter.
TIPS FOR EARLY ADOPTERS
Tip No. 1. At the start of surgery, I ask the patient to actively turn their head away from me because this produces more rotation than if the patient’s head is passively turned. Additionally, I position the table to the highest level so that my arms are positioned above my waist level. This reduces rotation of the eye away from me as there is less tendency to push down due to the arm position.
Tip No. 2. Using a gonioprism intraoperatively can take a while to master. During the OMNI procedure, a good view with identification of pigmentation and the line of blood reflux in the Schlemm's canal is essential. The latter is important because the lack of visible blood can indicate that the anterior chamber has been overfilled with OVD, compressing the Schlemm’s canal. I often fill the anterior chamber until the OVD is just about to overflow from the main wound. The view of all three bands of the angle (ie, trabecular meshwork/blood reflux line, scleral spur, and ciliary body band) must be visible (Figure 2). If only a single band is visible, further rotation of either the patient’s head or the microscope is needed. I am right-hand dominant, and I prefer a left-handed gonioprism. I find that gently resting the knuckle of my little finger on the patient’s nose or forehead while placing the gonioprism on the cornea prevents direct pressure from being applied to the cornea (Figure 3). Too much pressure can cause corneal striae and burping of viscoelastic out of the wound, providing a poorer view and a shallower anterior chamber to work with. There are also options for disposable hands-free gonioprims to facilitate a better view.
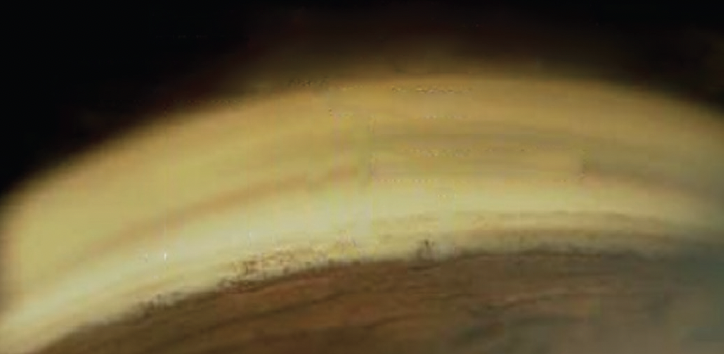
Figure 2. The view of all three bands of the angle (ie, trabecular meshwork/blood reflux line, scleral spur, and ciliary body band).

Figure 3. Fingertips are used to support the gonioprism.
Tip No. 3. Patient selection for your first few cases is crucial. Avoid using OMNI for the first few cases in phakic patients, eyes with a poor view of the angle, and in patients who present with any of the following:
- Corneal arcus or corneal scar;
- Corneal edema from complicated or prolonged cataract surgery;
- Smaller eyes with shallow anterior chamber; and
- Poor neck mobility.
As you are getting comfortable with the procedure, be cautious at the end of trabeculotomy in the eyes of patients on blood thinners. I find that leaving the anterior chamber hyperinflated can avoid any ongoing hyphema. I would also place a stitch in the corneal main wound if it is not watertight.
Tip No. 4. Tactical feedback with the device is important. I like the fact that the OMNI doesn't allow you to enter Schlemm’s canal in the wrong position—it visibly bounces back because it is a flexible microcatheter. On the other hand, once the trabecular meshwork is scored and the microcatherer is seated within the canal, it advances smoothly. Should I feel an obstruction while advancing the microcatheter, I simply rewind the wheel slightly as the OVD disperses down the canal to dilate it. I would then try to advance the microcatheter again. If the obstruction does not clear with the OVD, I would not attempt to push through because it risks catheter misdirection.
Tip No. 5. In my first few cases of trabeculotomy, there was a learning curve for achieving the right amount of tension in the microcatheter. There was too much slack in the microcatheter, and I was only achieving around 90º of a trabeculotomy at a time. I learned that the way to achieve the tension needed to produce an efficient 180º trabeculotomy was for the microcatheter to follow the corneal curvature closer to the angle.
Tip No. 6. Perhaps the most important tip is to learn how to manage patient expectations. This is especially important for patients who are undergoing a combined cataract surgery/MIGS treatment. Many times, they expect their vision to be exceptional after surgery—which it still can be—but they must understand that their vision might not be as crisp immediately postoperatively after a combined procedure. I like to tell these patients that they might experience blurry vision for 1 to 2 days because of the bruising in the eye.
CONCLUSION
The OMNI Surgical System is a fantastic option to treat outflow resistance, wherever it may occur, in the conventional outflow pathway. True to the MIGS paradigm, the procedure is efficient. The reduced risk profile is accomplished with no device implantation. In my experience, the pressure drop is efficient and predictable. The OMNI is a staple addition to the armementarium of a glaucoma surgeon.