

In our Smile Eyes Clinics, patients have had access to the latest laser vision correction surgical procedure via small incision lenticule extraction, or SMILE, since 2012. This procedure is attractive to many types of patients because it can be performed with one laser system, the VisuMax femtosecond laser (ZEISS), and because instead of requiring a flap in the cornea it only requires a keyhole incision through which a lenticule of tissue is removed.
The percentage of SMILE treatments we perform has steadily increased over the past 5 years, from 52% in 2012 to 67.6% in 2016. Because of this, and because the procedure has less capital investment and per-procedure costs to both the practice and the patient, the impact that SMILE has had on our revenue stream has been quite significant (Figure 1).
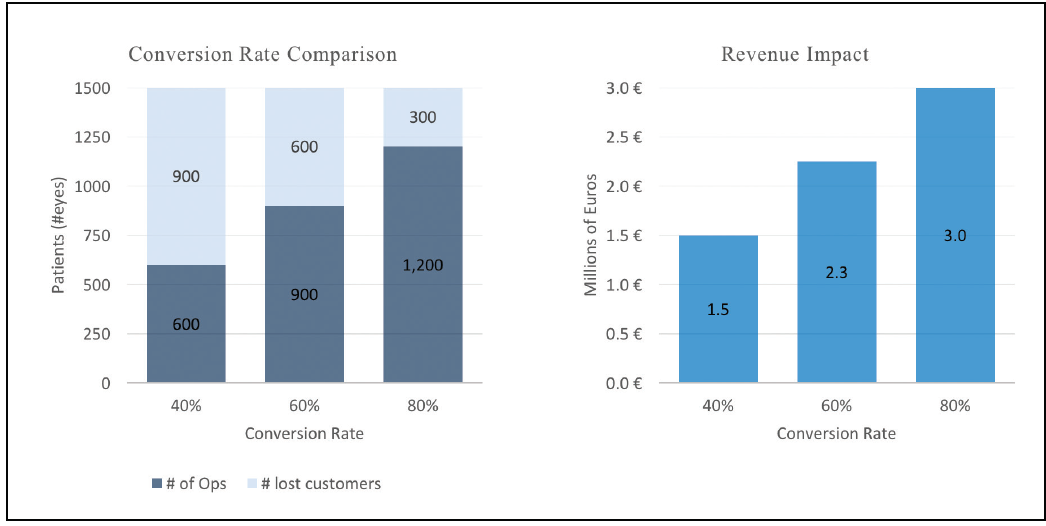
Figure 1. Conversion rate to SMILE and the impact on revenue at Smile Eyes.
STRUCTURE YOUR PROCESS
Part of the reason we have seen continued success and rising patient acceptance of SMILE in particular is that we use a structured patient counseling process. In 10 simple steps, patients can be both educated on SMILE and counseled on why the procedure is right for them.
Step No. 1: The opening. During the initial conversation with the patient, it is important that he or she receives a warm welcome to the practice. We always ask, “Who should we thank for the referral to our practice?” This can be used to create a connection with the patient and also provide insight into why he or she is interested in SMILE. Also during the first dialogue, we start the patient’s file and go over specific treatment plans that we offer.
Step No. 2: What can we do for you? Using an open-ended question like this can give the patient the opportunity to articulate exactly what it is that he or she is looking for in a treatment. The most common answer we hear is, “Because I want to get rid of my glasses.”
Step No. 3: Ask a follow-up question. That simple statement—“Because I want to get rid of my glasses.”—does not provide enough information to select the best procedure for the patient. Therefore, it is important to follow-up with, “Can you tell me why?” During this point in the patient counseling process, the patient should be doing 80% of the talking, and the clinician should listen and only lead the conversation when necessary. Throughout the process, the clinician must encourage positive thinking and provide a safe space for the patient to talk freely.
Step No. 4: Gauge the patient’s knowledge base. Has the patient done research on the internet? Has he or she heard about SMILE from family or friends? Has he or she seen brochures, visited a competitor, or attended an informational session about the procedure? Eliciting this information can help the surgeon to learn more about the patient, including the way he or she thinks about the procedure and what his or her fears are. This information also provides insight into the success of our marketing and into which marketing tools are successful and which are not.
Step No. 5: Determine and explain the patient’s suitability. An ocular examination including corneal tomography is a great tool to explain the suitability of the patient for laser vision correction. Symmetry of the topography, corneal thickness, and the traffic light appearance of the Belin Ambrosio tool (Figure 2) are easy for the patient to understand when explained properly. This understanding ensures the patient that there is a clear rationale why he or she is a good candidate for refractive surgery.
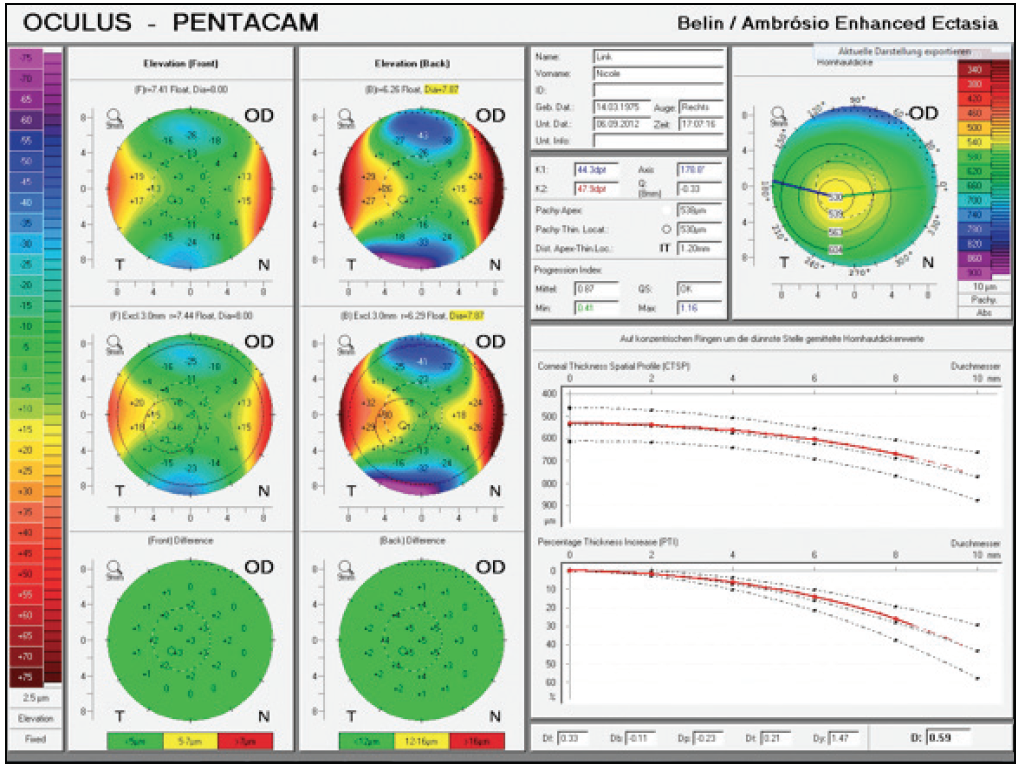
Figure 2. The Belin Ambrosio tool on corneal topography.
Step No. 6: Introduce the procedure in more detail. Once it is decided that the patient is a good candidate for SMILE, the clinician should then provide a thorough introduction to the procedure. At Smile Eyes, we like to provide a complete overview on the evolution of laser vision correction, from microkeratome LASIK to femtosecond LASIK to SMILE. It gives the patient a sense of how far refractive surgery has come and how we take years of knowledge and experience into account when selecting the right procedure for him or her. At this point in the counseling process, we ask that the patient watches a video about SMILE as another means of educating him or her about the procedure. This is important because some patients are visual learners. The key point here is the principle of evolution and not revolution in the technology. I always make it clear to patients that the basic principle of tissue removal has not changed since the beginning of laser vision correction. The only thing that has improved dramatically is the way in which we achieve this goal.
One mistake that can be made when being too enthusiastic about a new procedure is that the older procedures are pinned as negative. Instead, we should make it very clear that laser vision correction has always has been successful and reliable and has even continued to improve over the years.
Step No. 7: Identify the risks. We always suggest to the patient what procedure we think is best for him or her. But no matter what procedure the patient selects, an essential part of the counseling process is identifying the risks associated with the procedure. With SMILE, those risks include infection, suction loss during the procedure, postoperative refractive errors, dry eye, and the presence of halos or glare after surgery. We are also sure to let patients know that the risk of infection is extremely small and that all of the other risks have an easy solution.
Step No. 8: Take time to answer any questions. All patients have some fear surrounding refractive surgery. Taking the time to ask if the patient has any questions and to acknowledge that it is OK to feel nervous or anxious about surgery can go a long way in reassuring patients. Talking about the reality of fear with the patient and letting him or her voice any specific concerns is a great way to reinforce the trust that has been built between you. One thing that I have found helpful is to site a recent study by Kezirian et al,1 which showed that refractive surgeons are more than four times more likely to have had refractive surgery than the general population and that 91% have recommended refractive surgery to their immediate family members.
Step No. 9: Schedule the procedure. Once the patient has had the opportunity to ask questions, it is now time to schedule the procedure. At this point, it is best if the clinician leads the conversation. Ask, “When would you like to have surgery?” and give him or her the choice of different appointment dates and times.
Step No. 10: Closing. Confirm the appointment time with the patient, and then provide reassurance that he or she is making the right decision. Easing patient fears and providing positive dialogue at this stage strengthens the patient’s feelings about the procedure.
CONCLUSION
In the past 6 years, we have seen significant gains in the volume of SMILE procedures we have performed and in the profitability that our clinic has enjoyed. In fact, we have seen a 10% gain in our laser vision correction volume since offering SMILE. In order to ensure we can maintain the momentum we have created behind this procedure, we believe that following a structured patient counseling process like the one described here is necessary.
1. Kezirian GM, Parkhurst DG, Brinton JP, et al. Prevalence of laser vision correction in ophthalmologists who perform refractive surgery. J Cataract Refract Surg. 2015;41:1826-1832.
